
Dr. T. Ganesh honored with the Dr. Ramaiah Naidu Memorial Oration Award at the AMPICON 2024
The Ramaiah Naidu Memorial Oration (RNMO) Award was instituted by the Association of Medical Physicists of India (AMPI) in 1992 in the honor of pioneer Indian medical physicist Dr. Ramaiah Naidu. The oration award consists of a citation and a silver plaque. As per the norms of AMPI, the recipient of the RNMO award shall be a person of national/ international repute in the field of medical physics and is selected by the Executive Committee of AMPI.

For the year 2024, this most prestigious honor was bestowed on Dr. T. Ganesh for his long and distinguished services in the field of medical physics extending over four decades. Dr. Ganesh delivered his oration at the time of the Annual Conference of the Association of Medical Physicists of India AMPICON-2024 that was held during Nov 8-10, 2024 in Hyderabad, India.
HPV Vaccination in South Asia: Progress, Challenges, and the Path Forward
Rajni Verma1 & Arun Chougule2
1Assistant Professor & Radiation Safety Officer, Department of Radiological Physics, SMS Medical College&
Hospital, Jaipur, India
2Dean and Chief Academic Officer, Swasthya Kalyan Group, Jaipur, Ex-Head & Sr. Professor, Department of
Radiological Physics, SMS Medical College& Hospital, Jaipur, India
Introduction
Human papillomavirus (HPV) is a leading cause of cervical cancer, a major public health issue worldwide. In South Asia—which includes India, Bangladesh, Nepal, Bhutan, Sri Lanka, Pakistan, Afghanistan, and the Maldives—the burden of cervical cancer is particularly high. This is largely due to limited screening initiatives, low vaccination coverage, and health system disparities. This article offers a comprehensive overview of the current status of HPV vaccination across South Asia, highlighting recent advancements, ongoing challenges, and strategic recommendations for enhancing vaccine uptake.
Cervical Cancer Burden in South Asia
According to the World Health Organization (WHO), South Asia contributes significantly to the global cervical cancer burden:
• India: ~127,000 new cases annually
• Bangladesh: ~8,068 new cases
• Nepal: ~2,824 new cases
• Sri Lanka: ~1,451 new cases
• Pakistan: ~6,108 new cases
These figures underscore the critical need for robust prevention strategies, particularly the widespread implementation of HPV vaccination.
HPV Vaccination: Country-wise Overview
Bangladesh
In December 2024, Bangladesh completed the final phase of a nationwide HPV vaccination campaign across all divisions, including Barisal, Chittagong, Khulna, Mymensingh, Rajshahi, Sylhet, and Rangpur. Approximately 5.6 million adolescent girls aged 10–14 were vaccinated, achieving a remarkable 93% coverage. The campaign effectively targeted both in-school and out-of-school girls, ensuring equity in access.
The HPV vaccine has now been integrated into Bangladesh’s routine immunization program, focusing on Grade 5 girls and 10-year-old girls not enrolled in school.
India
As of May 2025, India is actively working to include the HPV vaccine in its National Immunization Programme (NIP) Despite launching its indigenous vaccine Cervavac in 2022—an initiative expected to improve affordability and supply—nationwide coverage remains below 6%. Policy efforts are currently underway to establish a uniform rollout.
Sri Lanka
Sri Lanka introduced the HPV vaccine into its National Immunization Programme in 2017, targeting girls aged 10–14. Delivered primarily through school-based programs, the country has built one of South Asia’s most effective vaccination frameworks. As of May 2025, Sri Lanka maintains a national coverage rate of approximately 82%.
Nepal
Nepal has made significant progress in HPV vaccination. Following earlier pilot initiatives supported by GAVI [Global Alliance for Vaccines and Immunization], the vaccine is now being administered nationwide as part of the government’s strategy to reduce cervical cancer incidence. The program has shown
encouraging results, particularly in urban and semi-urban areas.
Pakistan
As of May 2025, Pakistan has yet to incorporate the HPV vaccine into its national immunization schedule. While small-scale pilot programs have been conducted and policy-level discussions are ongoing, a countrywide rollout remains pending due to political, financial, and awareness-related barriers.
Other South Asian Countries
• Bhutan: A regional leader with consistent >90% coverage through successful school-based
vaccination programs.
• Maldives: Recent government-led initiatives show promise for achieving high coverage in the near
future.
• Afghanistan: Faces serious challenges such as conflict, poor health infrastructure, and limited public
awareness, hindering vaccination efforts.
Key Challenges in HPV Vaccine Implementation
1. Limited Awareness: Many communities lack knowledge about HPV and its link to cervical cancer.
2. Cultural and Religious Misconceptions: Fears around promoting early sexual activity deter vaccine
acceptance.
3. High Vaccine Costs: Although costs have historically been a barrier, locally produced vaccines like
India’s Cervavac are shifting the landscape.
4. Weak Healthcare Infrastructure: Rural and underserved areas often lack the logistics for mass
immunization.
5. Policy Gaps and Political Will: Delayed policy adoption and insufficient government prioritization
remain major bottlenecks.
Recent Successes and Positive Developments
• Bangladesh: Achieved 93% coverage through inclusive, division-wide campaigns.
• India: Introduction of Cervavac is a significant milestone, expected to increase coverage.
• Nepal: Successful transition from pilot projects to national rollout.
• Bhutan: Continues to serve as a regional exemplar with sustained high coverage.
• GAVI Support: Instrumental in supporting demonstration programs in Nepal, Bangladesh, and
Pakistan.
Recommendations for Advancing HPV Vaccination in South Asia
• Develop and Strengthen National Policies: Formalize HPV vaccine inclusion in immunization
programs across all countries.
• Community Engagement: Involve educators, religious leaders, and healthcare professionals to build
trust and improve outreach.
• Public Awareness Campaigns: Dispel myths through targeted educational initiatives, especially in
rural areas.
• Affordable Vaccine Access: Encourage public-private partnerships and leverage local manufacturing
to reduce costs.
• School-Based Delivery Models: Proven to be highly effective; should be replicated across the region.
• Monitoring and Evaluation: Invest in data systems to track coverage, identify gaps, and inform
policy decisions.
Conclusion
HPV vaccination presents a transformative opportunity to reduce cervical cancer incidence across South Asia. While countries like Bangladesh, Bhutan, Nepal, and Sri Lanka have made commendable progress, others such as India and Pakistan face persistent challenges. Accelerating progress toward WHO’s 2030 goal of eliminating cervical cancer as a public health problem will require political commitment, sustained funding,
community awareness, and regional collaboration.
References
1. World Health Organization. (2022). Cervical Cancer Country Profiles. https://www.who.int
2. International Agency for Research on Cancer (IARC). GLOBOCAN 2020. https://gco.iarc.fr/today
3. GAVI, the Vaccine Alliance. HPV Vaccine Programs. https://www.gavi.org
4. PATH. (2023). HPV Vaccination in South Asia: Lessons from Demonstration Programs.
5. Indian Council of Medical Research. (2023). Cervavac and Indigenous Vaccine Production.
6. Ministry of Health and Family Welfare, Bangladesh. (2024). National HPV Campaign Reports.
7. Ministry of Health, Sri Lanka. (2025). Immunization Program Data.
8. Ministry of Health and Population, Nepal. (2025). HPV Vaccine Implementation Update.
Local Manufacturing of Radiotherapy and Imaging Equipment: Opportunities and Challenges
Manoj K Semwal
Chief of Medical Physics and Radiological Safety, Army Hospital (R&R), New Delhi
It is often said that the 21st century belongs to Asia and in that specifically to South Asia in terms of economic growth and improvement in the standards of living. The reasons are not far to seek but the most obvious ones are the demographic advantage and the talented human resource that is available in this region. However, the success cannot be taken for granted despite the advantages. The onus is on the people living in this part of the world to make use of this window of opportunities. Medical and healthcare is one of the crucial sectors that is expected to play a significant role in not only directly contributing towards driving the economic growth but also act as a human resource enabler.
I have been part of the medical and healthcare sector for over three decades in India as a medical physicist engaged in clinical medical physics practice and in teaching & training of medical and para-medical radiation professionals. Planning and commissioning of radiation installations at government funded cancer centres also has been part of my professional work. The latter often involves choosing appropriate technology platforms for a centre within the existing financial resources. And almost always the suppliers of the technologies are based outside this part of the world. The imported medical technologies have been satisfactorily serving the interests of the patients over the years despite their high costs. Ruggedness and stability of performance of these radiotherapy and imaging systems have been responsible for providing reasonably adequate quality of care to the needy despite excessive patient load on them, especially in public hospitals. Of course, not without the well-trained and dedicated manpower. However, it is a fact that this level of care does not reach a large segment of population which is economically weaker and lives far away from the cities. There are over 800 medical linear accelerators including CyberKnife and TomoTherapy systems, two medical proton accelerators, about 160 telecobalt units including Gamma Knife and about 375 HDR brachytherapy units apart from some manual brachytherapy facilities presently available in India. In terms of diagnostic facilities, there are about 11,000 CT scanners, over one lakh x-ray machines including C-arms, O-arms and interventional radiology units, about 500 nuclear medicine centres with varying levels of equipment and devices among gamma cameras, SEPCT and PET facilities, and 24 medical cyclotrons facilities (1,2). Almost all of these facilities are concentrated in the cities. It is estimated that more than half of the 1.4 billion population of India still lives in villages where connectivity is not as good as in the cities. I must add that the information about radiation facilities in India is expected to represent the scenario in the entire region with minor variations in terms of availability of the facilities per million population.
There is unanimity among healthcare policy makers that with increasing cancer burden and awareness among the population the demand for radiation therapy and diagnostic equipment is rapidly increasing. Meeting the demand from imported equipment may prove to be difficult and costly. That is where the opportunities and challenges for indigenous manufacturing exist. Opportunities because there is a market and an ever-improving manufacturing ecosystem, and challenges because quality of the product needs to be of international standards. Radiation safety is added concern with such equipment. Along with the treatment delivery and imaging equipment, the equally important segment is radiation measuring and monitoring devices, and treatment planning systems (TPSs). India has been designing and manufacturing radiation monitoring devices based on Geiger Muller counters for a couple of decades. Ion-chamber based dosimeters (thimble and well-type) and TPSs have also been developed and manufactured. X-ray imaging systems too are being manufactured locally.
For radiation generating or radioactive source-based equipment used for imaging and treatment, there are well laid down safety requirements and regulations mandating type approval or certification of the equipment and technology. Atomic Energy Regulatory Board (AERB) in India is engaged in such certification from radiological safety point of view. Other than radiation safety aspects such equipment need to pass regulations for electrical & mechanical safety and functional performance as well. However, as on today, there are no such requirements or provisions for radiation monitors, dosimeters, TPSs, etc., in India. This situation needs to change as radiation monitoring and measuring devices, planning systems and similar accessories play an equally important role in the safe, accurate and optimised patient care. Creating the infrastructure for certification processes need synergy between various stakeholders such as certification/regulatory bodies, laboratories/testing facilities to realize standards, and users.
Medical Physicists in this region have a great opportunity to expand their horizons beyond clinical practice and get involved with research and development (R&D) and testing and validation of indigenous technologies. They can become involved in supporting the concerned certifying agencies in formulating the standards and certification processes. The support can be at individual levels or as part of professional medical physicist bodies. AMPI has, of late, been involved with the concerned government agencies for the purpose. In near future, we would like to be more intensely involved in the development of local technologies and establishment of the standards and associated processes.
References
- AERB Annual Report 2022
- G Sahani. Presentation at 12th International Patient Safety Conference. New Delhi, 21-22 Feb 2025.
Journey at Western Chapter Association of Medical Physicists
of India Conference 2025 (AMPICON WC-2025): Current
Trends, Future Prospects & Career Insights in Radiotherapy
Shriram Rajurkar
Assistant Professor, Department of Medical Physics, CIR, D. Y. Patil Education Society, Kolhapur, India
29th May 2025:The Department of Medical Physics, Centre for Interdisciplinary Research (CIR), D. Y. Patil Education Society (Deemed to be University), Kolhapur organized the Western Chapter Association of Medical Physicists of India Conference 2025 (AMPICON WC-2025) in association with the Association of Medical Physicists of India. The event was held at Sayaji Hotel, Kolhapur, on 26th and 27th April 2025, in collaboration with Kolhapur Cancer Centre, Shri Siddhivinayak Ganapati Cancer Hospital, Aster Aadhar Hospital, Horizon Hospital, and Shiv Cancer Institute.
The inauguration ceremony took place on 26th April 2025. Padmashree Awardee Dr. Shivram Baburao Bhoje, former Indian Nuclear Scientist, was the Chief Guest. In his address, Dr. Bhoje shared insights on the health impact of lung cancer among workers from mining areas and emphasized the advancements in radiotherapy for cancer treatment. The ceremony was chaired by Prof. Dr. C. D. Lokhande, Dean of Research, CIR, D. Y. Patil Education Society.
The dais was graced by WC-AMPI Chairman Dr. Rajesh Kumar, Organizing Committee Chairman and Dean of CIR Prof. Dr. C. D. Lokhande, WC-AMPI Secretary Mr. Rahul Phansekar, WC-AMPI Treasurer Mr. Anand Jadhav, WC-AMPI Organizing Secretaries Dr. Asawari Pawaskar and Dr. K. Mayakannan, and WC-AMPI Convener Mr. Thirunavukkarasu Mani. The conference witnessed participation around 250 delegates, including esteemed faculty from AERB, BARC, and medical physicists from across India.
During the conference, the scientific presentations covered advanced techniques such as dual-energy CT, MR LINAC, and new developments in image synthesis and artificial intelligence. Interactive panel discussions were conducted on topics like software based patient specific quality assurance (PSQA), total body irradiation (TBI), and total marrow and lymphoid irradiation (TMLI). AMPICON WC-2025 provided a valuable platform for networking with leading vendors and medical physicists from all over India.
On 27th April 2025, a specialized workshop on TBI and TMLI was conducted at Kolhapur Cancer Centre. Hands-on training during the workshop was provided by Mr. Thirunavukkarasu Mani, offering practical insights into advanced radiotherapy techniques.

SCMPCR HW-08 as a successful episode of SCMPCR handson training program: BPKMCH, Bharatpur, Chitwan, Nepal
Suresh Poudel1, Md Anwarul Islam2, Hasin Anupama Azhari2, Ranjanbhakta Bhandari1, Surendra Bahadur Chand1, Shivaji Poudel1, Golam Abu Zakaria2
1B P Koirala Memorial Cancer Hospital, Bharatpur, Chitwan, Nepal
2South Asia Center for Medical Physics and Cancer Research, Dhaka, Bangladesh
South Asia Center for Medical Physics and Cancer Research (SCMPCR), Dhaka, Bangladesh under the leadership of Prof. Dr. Golam Abu Zakaria and management of Prof. Dr. Hasin Anupama Azhari has made its place as a successful organization for organizing various scientific activities, e-learning program, hands-on workshops conducted on a regular basis etc. It has gathered wide appreciation from different societies and
organization for its causes.
As SCMPCR is taking off its activities beyond Bangladesh, and after successful organization of SCMPCR HW-07 in February 2024 at Kolkota, India, this time SCMPCR hands-on workshop (SCMPCR-HW08) was held between 13th to 16th March, 2025 at B P Koirala Memorial Cancer Hospital (BPKMCH), Bharatpur, Chitwan, Nepal. It was an episode of a series of hands-on workshop SCMPCR organizes each year in different countries in South Asia. The program was a wonderful example of collaborative effort of SCMPCR and BPKMCH in co-operation with Nepalese Association of Medical Physicists (NAMP), which catered the need of international and national participants and satisfied trainers with great honor and hospitality. The title of the workshop was “Clinical Implementation of SRS, SRT and SBRT for Medical Physicists and Radiation Oncologists”. It was an EBAMP accredited course for 38 CPD points.
BPKMCH is the largest government funded comprehensive cancer hospital in Nepal. It is equipped with three medical linear accelerators (Varian Truebeam, Clinac iX and 600 CD), a HDR brachytherapy unit and a CT simulator. There are seven radiation ncologists, six medical physicists, thirteen technicians, and two onconurses in the department of radiation oncology, of which the current head of epartment is Dr. Ranjanbhakta handari and Mr. Surendra Bahadur Chand is in-charge of medical physicists. It offers a range of treatment services like 3DCRT, IMRT, VMAT and IGRT. It treats 200 patients each month, and its staff members are trained in different countries and dedicated in patient services. Also BPKMCH is known for hosting different national and international seminars, conferences, and has praiseworthy amenity and ambiences.
The four-day workshop was a well organized effort of the organizers, which had both the theoretical and practical components, delivered by eminent speakers from six different countries (Germany, Belgium,
Netherlands, Switzerland, Bangladesh and India) and two medical product vendors (Siemens Healthineers and PTW). Forty-two participants (Medical Physicists, Radiation Oncologists and RTTs) from three different countries (Bangladesh, India and Nepal) attended the program with great enthusiasm. There were participants from almost every cancer hospital in Nepal. As new machines with advanced features are being installed in Nepal, this particular training program was important to shed nowledge on SRS, SRT and SBRT to local participants, and empower with wider knowledge and skills to foreign participants. Before the formal program begun, some physicist colleagues from Kathmandu displayed their hospitality by welcoming speakers at Tribhuwan International Airport in Kathmandu and accompanying them to their hotel in Chitwan.
On 13th March, the first day of the program, the event started with a registration process at 8:30 am at Hall Room, BPKMCH, while the formal training program begun at 10:30 am with the introductory lecture on SRS, SRT and SBRT by Dr. Raju Srivastava, Belgium. This was followed by lecture by Prof. Dr. Sarbani Ghosh Laskar, India on Head and Neck delineation and associated issues, while Dr. Robert Semrau, radiation oncologist from Germany discussed on impact of contouring on quality of treatment plans. A lunch at Chitwan Garden Resort offered with traditional Nepalese cuisine to participants and speakers was a nice opportunity to everyone to get introduced to each other. It was further followed by a follow-up lecture by Dr Semrau on imaging modalities, image registration and pitfalls. Additionally, two online lectures- hypofractionation for
breast cancer by Dr. Janine Simons (Netherlands) and hypofractionation for prostate cancer by Prof. Luca Incrocci (Netherlands) added a flavor to novel purpose of the event.
The second day program kicked off with an enlightening lecture by Dr. Sarbani on radiological challenges in SRS, SRT and SBRT, which was followed by a motivating lecture by Prof. Dr. Golam Abu Zakaria on Physics
Quality Assurance, while after a short tea break, Ms. Tanya Bahl ( Varian) shared ideas on 4D CT scanning, MR fusion and RGSC for Advanced treatment planning, and Dr. Binay Shrestha (Switzerland) through his online lecture discussed plan evaluation and clinical protocols in relation to SRS, SRT and SBRT. After the lunch at the traditional Thakali Kitchen, once again Ms. Bahl spoke on plan optimization and algorithms for SRS, SRT and SBRT dose calculation. The final lecture for the day was delivered by Dr. K. Kanakavel (PTW), who shed light on patient specific QA with various QA devices. The scientific program ended at 4:30 pm. Following that the formal inauguration session was held at Chitwan Garden Resort.
The session started at 6:30 pm, in the glorious presence of the chief guest Prof. Dr. Anjani Kumar Jha, ViceChairperson of Nepal Medical Council, the apex body of medical education in Nepal. Also Dr. Bijay Raj Neupane, Chairman, BPKMCH, Board of Directors, Dr. Shivaji Poudel (Executive Director, BPKMCH),
former BODs, Deputy Director, HoDs (BPKMCH), other staff members, invitees, and media personnel added to the glory of the session. Dr. Jha praised the role of medical physics in healthcare settings, and emphasized on the necessity of medical physics education in Nepal. His ppreciation to SCMPCR, BPKMCH and NAMP to organize such events in Nepal was noteworthy. Similarly, Prof. Golam Abu Zakaria (Chairman SCMPCR) during his speech emphasized his interest to extend SCMPCR programs in other countries in South Asia. He also asked all the participants to contribute to SCMPCR newsletter in the form of scientific articles. He added that the newsletter has grown and acts as a nice platform for the physicists in the region to express their views
on various issues related to medical physics and radiation oncology, thus increasing their global visibility through their write-ups. He further assured that the SCMPCR will support BPKMCH in the clinical implementation of newer techniques. Other speakers highlighted the importance of such collaborative efforts
to uplift the radiation services in Nepal. Prof. Dr. Hasin Anupama Azhari shared the success of SCMPCR in various arena and its effort to realize the novel dream of strengthening medical physics education for quality health services in South Asia.
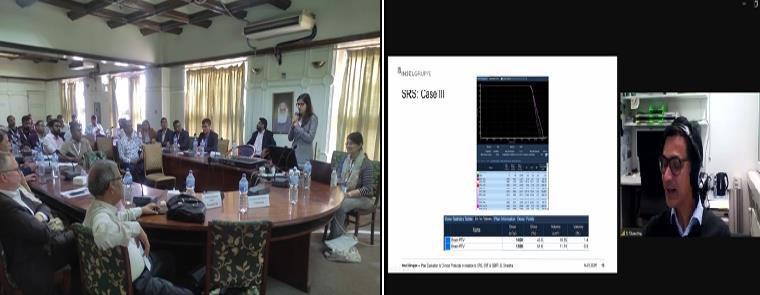
On the third day, the participants gathered at the radiotherapy building of the hospital and were divided into two groups: the first group of radiation oncologists was led by Dr. Laskar and Dr. Semrau and the second group of medical physicists and RTTs was led by Dr. Raju Srivastava, Dr. K Kanakaval and Ms. Tanya Bahl. The first group polished their skills on contouring, plan evaluation, image fusion and contouring on 4DCT
while the second group performed practical tutorials on patient specific QA with particular focus on isocenter verification through Winston-Lutz test using ball bearing and PTW software and learned various data analysis techniques. There were coffee and lunch breaks in between. The day ended with a general discussion on the role of medical physicists in clinical context. It was a fruitful day with opportunities for participants to learn
things practically.
On the final day, at Hall Room, two separate groups (of radiation oncologists and medical physicists &RTTs) were formed to whom two different sets of question papers were given to evaluate learning outcomes. Except
few participants, almost everyone passed the exam to gather EBAMP CPD points. This reflects the success of the training program, which the implementation of SRS, SRT and SBRT at their respective hospital will truly make the event successful. SCMPCR will remain in contact with them to get the regular feedback even after
the event.
Moreover, participants and speakers enjoyed the natural beauty of Chitwan, and many of them took opportunity to visit Royal Chitwan National Park and could observe Elephant Breeding center there, onehorned rhinos, alligators, deers, peacocks and other wild animals. To sum up, participants and speakers
experienced the true blend of scientific activity and natural beauty of Chitwan alongside the hospitality
provided by BPKMCH, particularly by the Dr. Shivaji Poudel, Dr. Ranjanbhakta Bhandari (HOD, Radiation Oncology), Mr. Surendra Bahadur Chand (RSO), radiation oncologists, medical physicists and other staffs, during the program and beyond was extraordinary.
Prof. Arun Chougule Awarded Prestigious IUPESM Fellowship

We are pleased to announce that Professor Arun Chougule has been awarded the prestigious IUPESM Fellowship, one of the highest international honors in the field of healthcare improvement through science, technology, and biomedical engineering.
The Fellowship of the International Union for Physical and Engineering Sciences in Medicine (IUPESM) recognizes individuals whose sustained and high-impact contributions have significantly advanced the profession
at both national and international levels.
Selection as an FIUPESM is a lifetime honor that reflects Professor Chougule’s exceptional dedication to the global progress of health sciences through technology and physics. It places him among an elite group of international leaders committed to advancing human health through scientific excellence.
Candidates for this prestigious fellowship are selected based on:
• Sustained, high-impact contributions to the field at both national and international levels.
• Leadership in research, education, or the development of health technology.
• Advancing the goals of healthcare improvement through science and technology.
• Peer recognition and dedicated service to professional organizations such as the International Organization for Medical Physics (IOMP), the International Federation for Medical and Biological Engineering (IFMBE), and IUPESM itself.
- The IUPESM Fellowship aims to:
• Recognize outstanding contributions to the advancement of physical and engineering sciences in medicine globally.
• Honor excellence in research, leadership, education, innovation, and international service.
• Promote global collaboration, upholding the highest standards of scientific practice and ethical conduct in medical physics and biomedical engineering.
Different Techniques of Radiotherapy for Breast Cancer
Md Mokhlesur Rahman1
, Shadia Tun Nayeem1
1Gono Bishwabidyalay (University)
Preface: Among the all other cancers for women, breast cancer is still leading the malignant tumor. This cancer usually starts in one area and gradually spreads with a predictable pattern to nearby lymph nodes and blood vessels, eventually affecting the rest of the body. In earlier treatment approaches, doctors recognized that removing the main tumor was not always enough because microscopic cancer cells could still remain. To address this, radiation therapy was either used alongside surgery to eliminate leftover cancer cells or chosen instead of surgery when operating was not practical due to location or concerns about appearance and function. [1].
Phases: For the adjuvant and non-adjuvant phases, many treatment comparisons show a 10–25% reduction in breast cancer mortality and recurrence, with no increase in non-breast-cancer deaths. However, certain therapies pose additional risks. Radiotherapy increases mortality risks linked to heart disease, lung cancer, and esophageal cancer, with severity correlating to radiation doses received by these organs [2]. And compared to standard radiotherapy, concurrent chemoradiation increased pCR rates (14% vs 22%, P<.001) but showed no significant difference in disease-free (69% vs 81%, P=.186, HR 0.51) or overall survival (74% vs 89%, P=.162, HR 0.46) at 3 years. Toxicity included 25% pneumonitis, 25% dermatitis, and one death from a study of Muriel Brackstone et al. [3].
- Non-Adjuvant: Non-adjuvant/neo-adjuvant radiotherapy is given before primary treatment to shrink tumors, improving surgical success. It may boost disease-free survival without affecting overall survival, especially in estrogen receptor-positive early-stage breast cancer patients [4].
- Adjuvant: Adjuvant radiotherapy, given after surgery in women under 50 with early-stage breast cancer, reduces recurrence risk by eliminating residual cancer cells. Factors like cancer type, stage, and lymph node involvement guide treatment, though cardiac toxicity is a concern for left-sided breast cancer due to heart proximity [5].
- Concurrent: Concurrent radiotherapy, combined with chemotherapy, improves treatment for locally advanced breast cancer (LABC) that is inoperable. Studies show higher response rates with concurrent chemoradiotherapy (CCRT) compared to systemic therapy alone, making it a potential option when neoadjuvant approaches are less effective [6].
Types: Depending on how the radiotherapy is given, treatment type has two forms.
EBRT: External Beam Radiation Therapy (EBRT) delivers radiation from outside the body to the targeted area, typically following breast-conserving surgery (BCS) or mastectomy. It focuses on treating the whole breast, chest wall, and sometimes nearby lymph nodes to eliminate remaining cancer cells and reduce recurrence risk. Treatment usually typically given daily, five days a week, for 6 to 7 weeks. A shorter, more intense course called accelerated radiation may last 3 to 4 weeks [7].
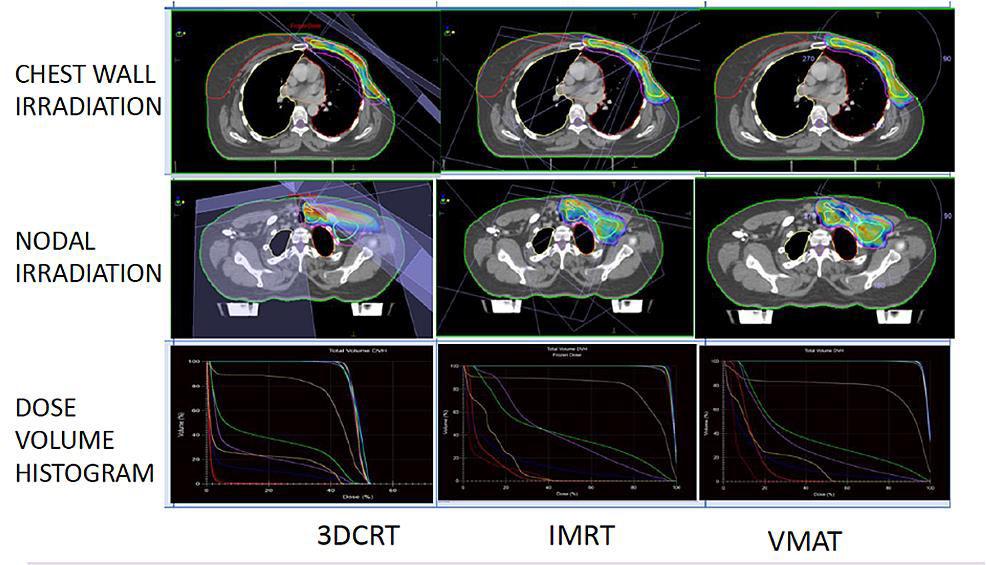
Modalities: From the most commonly used modalities, study shows that both IMRT and VMAT demonstrates superior conformity compared to 3D-CRT, with increases of 27% and 30%, respectively. Additionally, inverse planning techniques (IMRT and VMAT) provides more homogeneous dose distributions (10% improvement) and reduced hotspots (14% reduction) relative to 3D-CRT [8].
- 3DCRT: 3DCRT utilizes three dimensional images to plan and uses forward treatment planning where dose distributions are calculated after given beam parameters.
- IMRT: A developed form of 3DCRT where by the beam modulation with MLC the intensities are calculated to provide the given objectives and constraints on dose distributions to the target volume and organs at risk (OARs).
- VMAT: First it was IMAT, which worked on the gantry rotation to modulate the beam intensities with the same dose rate and when the dose rates were changed along with gantry rotation, it became VMAT.
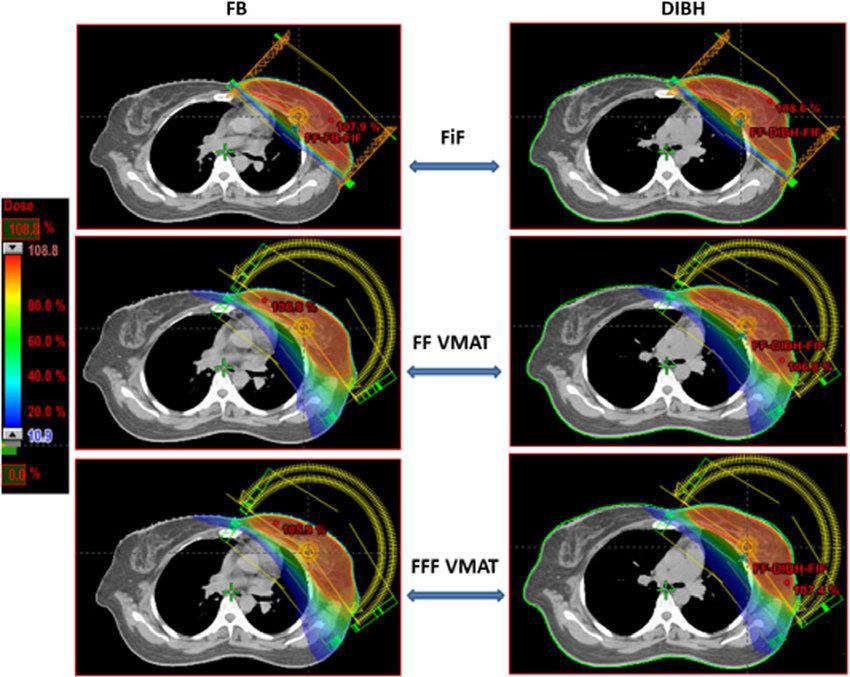
Techniques: Cardiac morbidity and pulmonary problems are considered as risks in breast treatment. A comparison between irradiated and non-irradiated patients revealed a significant rise in mortality rates, primarily due to heart disease and lung cancer, with rate ratios of 1.27 and 1.78, respectively [9]. Study results imply that the dose of the heart, left anterior descending (LAD) aretery and ipsilateral lung in the deep- inspiration breath-hold (DIBH) group was significantly lower than that in the free-breathing (FB) group as DIBH modifies the volume of considered OARs [10].
- FB: Free Breathing, where patients breath normally during treatment that ensures fast treatment delivery.
- DIBH: Deep Inspiration Breath Hold, where patient takes a deep breath and holds it, expanding the chest and moving the heart away from the breast/chest wall.
BT: Brachytherapy is a radiation technique where radioactive sources are placed directly into or near the target tissue. Currently, brachytherapy-based accelerated partial breast irradiation (APBI) is the only method with level 1 evidence, supporting its use as a viable alternative to whole breast irradiation (WBI) following breast- conserving surgery (BCS) for patients with low-risk, early-stage breast cancer [12].
Modalities: Among the brachytherapy modalities for breast cancer, intra-operative radiotherapy (IORT) is convenient than the conventional brachytherapy that includes intracavitary and interstitial brachytherapy procedure for low risk breast cancer conserving the breast [13].
- IORT: A precise partial breast irradiation (PBI) technique that delivers a single 10-30 Gy dose to the tumor bed during surgery. It can serve as sole RT or a boost, targeting the lumpectomy cavity (1-2 cm margin). Risk-adapted IORT can replace whole-breast radiotherapy (WBRT) for low-risk breast cancer (BC), while high-risk BC may still require WBRT based on histopathology [14].
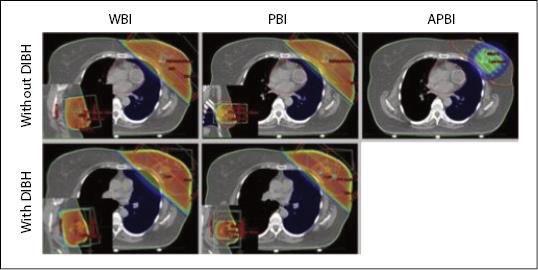
Techniques: Compared to WBI of external beam radiation therapy, PBI/APBI showed higher local recurrence rates (HR 1.62), worse cosmesis (OR 1.51), and increased late toxicity, including fibrosis, telangiectasia, and fat necrosis. Acute skin toxicity was lower (OR 0.04), but new ipsilateral breast primaries were more frequent (OR 3.97). Overall survival remained unchanged (HR 0.90), with no significant differences in cause-specific survival, distant metastasis-free survival, relapse-free survival, loco-regional recurrence-free survival, or mastectomy rates. Compliance exceeded 90%, though cost, quality-of-life, and patient preference data were lacking [15].
- PBI: Partial Breast Irradiation that delivers radiation to a limited area around the tumor, minimizing side effects and treatment duration.
- APBI: Accelerated Partial Breast Irradiation, is a faster version of PBI, typically completed in a shorter timeframe (often within a week).
End-Word: Studies show that women under 40 have higher recurrence rates after radiotherapy due to denser breast tissue, which affects radiation absorption. As fatty tissue increases with age, recurrence rates decline. And treatment effectiveness varies by type, modality, and technique, with tumor characteristics, radiation methods, chemotherapy regimens, and surgical approaches influencing disease control, survival rates, and side effects.
References:
[1] Julie A. Bradley, and Nancy P. Mendenhall, “Novel Radiotherapy Techniques for Breast Cancer,”
Annual Review of Medicine, vol. 69, pp. 277-288, January 2018.
[2] Amanda J. Kerr, David Dodwell, Paul McGale, Francesca Holt, Fran Duane, Gurdeep Mannu, Sarah
C. Darby, Carolyn W. Taylor, “Adjuvant and neoadjuvant breast cancer treatments: A systematic review of their effects on mortality,” Cancer Treatment Reviews, vol. 105, 03 March 2022.
[3] Muriel Brackstone, David Palma, Alan B. Tuck, Leslie Scott, Kylea Potvin, Theodore Vandenberg, Francisco Perera, David D’Souza, Donald Taves, Anat Kornecki, Giulio Muscedere, Ann F. Chambers, “Concurrent Neoadjuvant Chemotherapy and Radiation Therapy in Locally Advanced Breast Cancer,” Radiation Oncology: Biology, Physics, vol. 99, no. 4, pp. 769-776, 15 November 2017.
[4] Jan Poleszczuk, Kimberly Luddy, Lu Chen, Jae K. Lee, Louis B. Harrison, Brian J. Czerniecki, Hatem Soliman & Heiko Enderling, “Neoadjuvant radiotherapy of early-stage breast cancer and long-term disease-free survival,” Breast Cancer Reserarch, vol. 19, 30 June 2017.
[5] “Adjuvant therapy: Treatment to keep cancer from returning,” 28 May 2025. [Online]. Available: https://www.mayoclinic.org/diseases-conditions/cancer/in-depth/adjuvant-therapy/art-20046687.
[6] V Mandilaras, N Bouganim, J Spayne, R Dent , A Arnaout, JF Boileau, M Brackstone, S Meterissian, M Clemons, “Concurrent chemoradiotherapy for locally advanced breast cancer—time for a new paradigm?,” Current Oncology, vol. 22(1), pp. 25-32, February 2015.
[7] “Radiotherapy For Breast Cancer: Types, Success Rate, Side Effects And More,” 21 February 2025. [Online]. Available: https://oncodaily.com/oncolibrary/radiotherapy/radiotherapy-for-breast.
[8] Saroj Kumar Das Majumdar, Adhar Amritt, Sovan Sarang Dhar, Sandip Barik , Sasanka S Beura, Tushar Mishra, Dillip K Muduly, Ashish Dash, Dillip Kumar Parida, “A Dosimetric Study Comparing 3D-CRT vs. IMRT vs. VMAT in Left-Sided Breast Cancer Patients After Mastectomy at a Tertiary Care Centre in Eastern India,” Cureus, vol. 14(3), 28 March 2022.
[9] Thomas Madera ∙ Rachel Pacea ∙ Rui T. Boucas da Silvaa,d ∙ Lukas Erwin Johannes Adama ∙ Gabriela Näfa ∙ Christopher Charles Wintera ∙ Mania Maria Aspradakisa,d ∙ Marco Radovicb ∙ Aristotelis Spyridonidisa ∙ Stefanie Hayozc ∙ Brigitta Gertrud Baumert, “Deep inspirational breast hold (DIBH) for right breast irradiation: Improved sparing of liver and lung tissue,” Clinical and Translational Radiation Oncology, vol. 45, 22 January 2024.
[10] Yongkai Lu, Di Yang, Xiaowei Zhang, Yonggang Teng, Wei Yuan, Yuemei Zhang, Ruixin He, Fengwen Tang, Jie PangJie Pang, Bo Han, Ruijuan Chen, Yi Li, “Comparison of Deep Inspiration Breath Hold Versus Free Breathing in Radiotherapy for Left Sided Breast Cancer,” Front Oncology, vol. 12, 21 April 2022.
[11] Nagaraj Jagadheeskumar, Anu Radha Chandrasekaran, “Is it advantageous to use deep inspiration breath hold (DIBH) over free breathing for FAST-Forward dose fractionation scheme in treating carcinoma of left-sided breast? A dosimetric study,” Journal of Radiotherapy in Practice, 17 May 2021.
[12] Salvatore Cozzi ,Matteo Augugliaro,Patrizia Ciammella,Andrea Botti ,Valeria Trojani,Masoumeh Najafi,Gladys Blandino,Maria Paola Ruggieri,Lucia Giaccherini,Emanuele Alì, “The Role of Interstitial Brachytherapy for Breast Cancer Treatment: An Overview of Indications, Applications, and Technical Notes,” Cancers, vol. 14(10), 23 May 2022.
[13] Courtney Misher, “Brachytherapy for Breast Cancer,” Oncolink, 2025.
[14] Dr Sujata Sarkar, “Intra-Operative Breast Brachytherapy: Implementation and Clinical Considerations,” Apollo Multi-Speciality Hospital, Kolkata, India.
[15] Brigid E Hickey, Margot LehmanDaniel P FrancisAdrienne M See, “Partial breast irradiation for early breast cancer,” Cohrane Library, 18 July 2016.
[16] Igor Sirak, Denisa Pohanková, Linda Kašaová, Miroslav Hodek, Petr Motyčka, Ahmed Asqar, Jakub Grepl, Petr Paluska, Veronika Novotná, Milan Vosmik, Jiri Petera, “Cardiac doses with deep inspiration breath hold in breast cancer radiotherapy: direct comparison between WBI, PBI, and interstitial APBI,” Reports of Practical Oncology and Radiotherapy, vol. 29(2), pp. 155-163, 28 March 2024.
[17] Eleanor E. R. Harris, William Small Jr, “Intraoperative Radiotherapy for Breast Cancer,” Front Oncology, vol. 7, 22 December 2017.
BMPS organizes its 4th International Conference on Medical Physics in Radiation Oncology and Imaging (ICMPROI-2025)
Md. Mokhlesur Rahman¹, Rofikun Nahar Rosmi1
¹Department of Medical Physics and Biomedical Engineering, Gono Bishwabidyalay (University), Savar, Dhaka
The 4th International Conference on Medical Physics in Radiation Oncology and Imaging (ICMPROI-2025) was held from February 13 to 15, 2025, at BRAC University in Dhaka, Bangladesh. The event was jointly organized by the Bangladesh Medical Physics Society (BMPS) and BRAC University, in collaboration with the South Asia Centre for Medical Physics and Cancer Research (SCMPCR), and officially endorsed by the International Organization for Medical Physics (IOMP) and the Asia-Oceania Federation of Organizations for Medical Physics (AFOMP).

A Landmark Event for Global Medical Physics Collaboration: The ICMPROI-2025 marked a defining moment in the field of medical physics across South Asia and beyond, bringing together over 150 researchers, medical physicists, clinical professionals, and students from more than 15 countries. Themed “Medical Physics in Cancer Care: Challenges and Opportunities for International Cooperation,” the event focused on harnessing global partnerships to elevate healthcare standards in low- and middle-income countries.
Conference Highlights
- Opening Ceremony: Distinguished guests including Prof. Dr. Mohammad Anwar Hossen (Chief Guest, UGC Member), Prof. Dr. Syed Ferhat Anwar (VC, BRAC University), and international experts from the UCSF, NICRH, and AFOMP graced the opening.Prof. Dr. Golam Abu Zakaria, a pioneer in medical physics, delivered a powerful keynote on the global trajectory of cancer care and medical physics development.
- Scientific Program:
Over 15 technical sessions were held, covering areas like:- Artificial Intelligence in Radiotherapy
- Brachytherapy Innovations
- Medical Imaging and Diagnostic Technologies
- Radiobiology, Dosimetry, and Radiation Protection
- Education & Professional Development in Medical Physics
- Global policy frameworks and institutional roles

Eminent speakers included Prof. Tomas Kron, Prof. Chai Hong Yeong, Dr. Manju Sharma, and representatives from IOMP, AAPM, DGMP, and SCMPCR.
- Pre-Congress Workshop (Feb 12, CMH Dhaka): Hands-on training in SRS/SBRT, Small Field Dosimetry, Contouring, and End-to-End QA, delivered by world-class facilitators like Dr. Maria Mania Aspradakis and Dr. Manju Sharma.
- SCMPCR & AAPM Joint Session: Focused on transformative education models, regional training initiatives, and the expansion of tele-education and e-learning platforms in Asia and Africa.
- Poster & Vendor Exhibits: Showcased cutting-edge innovations from Varian, PTW, Radformation, and others, demonstrating AI-powered auto-contouring, adaptive radiotherapy, and SGRT.
Community and Cultural Exchange: The event concluded with a grand Cultural Program and Gala Dinner, celebrating diversity, innovation, and unity in global cancer care. The participation of young researchers and professionals underscored the growing strength of the next generation in medical physics.
ICMPROI-2025 served as a beacon of international cooperation, igniting meaningful dialogue and collaborative spirit. It reaffirmed Bangladesh’s and South Asia’s growing role in shaping the global discourse on medical physics, cancer research, and sustainable healthcare development.
Clinical Implementation of SRS, SRT, and SBRT Workshop:
Advancing Precision Radiotherapy in South Asia Held at B P Koirala Memorial Cancer Hospital, Nepal | March 13–16,2025
Dinesh Saroj
Medical Physicist & RSO-III, Balco Medical Centre, A unit of Vedanta Medical Research foundation, New Raipur, Raipur Chhattisgarh, India
In the rapidly advancing field of oncology, radiation therapy remains a cornerstone of cancer management. With increasing global emphasis on precision medicine, high-dose, hypo-fractionated stereotactic techniques like Stereotactic Radiosurgery (SRS), Stereotactic Radiotherapy (SRT), and Stereotactic Body Radiotherapy (SBRT) have become pivotal in treating small-to-moderate tumors, especially those situated in surgically challenging or anatomically sensitive regions such as the brain, spine, liver, and lung. These methods allow accurate tumor targeting with minimal exposure to surrounding healthy tissues, significantly improving patient outcomes.

At the heart of this advancement is the South and Central Asia Medical Physics Collaboration and Research (SCMPCR), whose vision is to build a robust network of medical physicists, clinicians, and researchers across the region. SCMPCR’s mission emphasizes capacity building, cross-border knowledge exchange, and the promotion of best practices in medical physics and radiotherapy. By supporting initiatives like this workshop, SCMPCR continues to bridge resource and expertise gaps, empowering healthcare professionals to deliver high-quality cancer care in diverse clinical settings.
Recognizing the urgent need to disseminate the clinical and technical knowledge required to implement these complex techniques, SCMPCR organized a Four-day international workshop at B P Koirala Memorial Cancer Hospital(BPKMCH) in collaboration with BPKMCH and NAMP. The event drew over 42 participants including medical physicists, radiation oncologists, and Radiation Therapist from India, Nepal, and Bangladesh, and featured distinguished faculty from India, Germany, Switzerland, Belgium, and the Netherlands.
Interdisciplinary Emphasis: Bridging Clinical Insight and Technical Expertise
One of the workshop’s key distinguishing features was its dual focus on both medical physicists and radiation oncologists. This inclusive format acknowledged that the successful implementation of stereotactic techniques relies on close collaboration between the clinical and technical teams. Whereas radiation oncologists make critical decisions about treatment eligibility, fractionation schedules, and anatomical targeting, medical physicists ensure accurate dose calculations, quality assurance (QA), and compliance with international safety protocols.
Unlike traditional training sessions that cater to only one discipline, this workshop offered parallel and collaborative sessions that emphasized clinical decision-making, contouring, treatment planning, dosimetry, QA, and image-guided verification techniques—all delivered in a structured and logically progressive format.

Day 1: Clinical Concepts and Anatomical Contouring.
Understanding the clinical rationale and anatomical considerations is essential for accurate implementation of SRS, SRT, and SBRT. Day 1 established foundational knowledge crucial for every step-in stereotactic workflow, from patient selection to target delineation
The workshop commenced with an inauguration ceremony graced by leadership from BPKMCH and SCMPCR, setting the tone for a high-caliber academic event. The first day focused on establishing a strong foundational understanding of stereotactic techniques and anatomical contouring essentials.
Dr. Raju Srivastava (Belgium) delivered the opening keynote, providing a comprehensive overview of the principles, indications, and limitations of SRS, SRT, and SBRT. He emphasized the importance of patient selection criteria, immobilization techniques, and the need for stringent imaging protocols to ensure sub- millimeter accuracy. Following this, Dr. S. Ghosh Laskar (Tata Memorial Hospital, Mumbai, India) led an in-depth session on contouring for head and neck SRT, focusing on high-dose conformity requirements and dose constraints for organs-at-risk (OARs). His session also featured real-world clinical cases, underlining the complexity of anatomical delineation in stereotactic settings.

Dr. Robert Semrau (University Hospital Düsseldorf, Germany) presented a session on the critical impact of contouring accuracy on dosimetric outcomes. His lecture emphasized the use of image fusion (CT-MRI, PET-CT), deformable registration, and the importance of inter observer variability reduction. He continued with a session on image guidance and registration pitfalls, drawing attention to the potential dosimetric consequences of inaccurate image alignment. In the evening, two online guest lectures broadened the clinical scope of the program.
Dr. Janine Simons (Netherlands Cancer Institute) presented the role of hypo-fractionation in breast cancer, highlighting trials like Fast-Forward and their implications for regional practice.
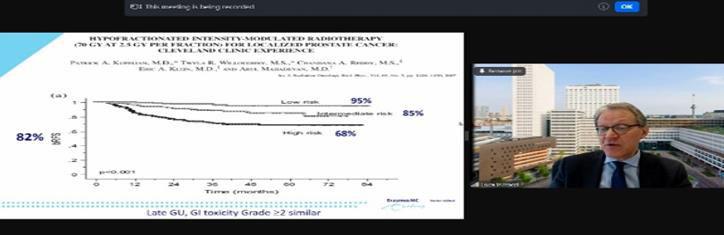
Prof. Dr. Luca Incrocci (Erasmus MC, Rotterdam) delivered a talk on ultra-hypo-fractionation in prostate cancer, covering evidence-based schedules like the HYPO-RT-PC trial and their application in resource- limited settings.
Day 2: Planning, Radiobiology, and Quality Assurance: Treatment planning and QA are cornerstones of safe stereotactic radiotherapy. Day 2 addressed the radiobiological principles behind hypo-fractionation, essential planning techniques, and the rigorous QA needed to ensure accuracy and patient safety.

Day 2 began with a powerful radiobiology session by Dr. S. Ghosh Laskar, who explained the Linear- Quadratic (LQ) model, Biologically Effective Dose (BED), and Equivalent Dose in 2 Gy fractions (EQD2) calculations—critical tools in evaluating high-dose-per-fraction treatments. She provided practical examples comparing SRS/SBRT plans with conventional regimens, enhancing participants’ ability to understand the radiobiological trade-offs.
Prof. Dr. Golam Abu Zakaria (Germany), a key figure at SCMPCR, provided an engaging lecture on
patient-specific QA methodologies, emphasizing gamma index analysis, absolute dose verification, and tools suited for stereotactic environments. He also discussed common challenges in QA workflows such as detector resolution, phantom design, and positioning reproducibility.
A significant highlight of the day was the session by the Varian Medical Systems representative, who presented an in-depth demonstration of HyperArc—a state-of-the-art technology designed to optimize SRS and SRT treatment planning. HyperArc automates and streamlines the planning of non–coplanar volumetric modulated arc therapy (VMAT) for cranial stereotactic radiosurgery.
It ensures ultra-conformal dose distributions, steep dose gradients, and minimal exposure to surrounding healthy tissues—all of which are critical for treating multiple or complex brain lesions. HyperArc reduces planning variability by automating beam arrangement and optimization parameters, allowing for consistent high-quality plans. Non-Coplanar Arc Delivery enhances dose conformity and sharpens falloff, especially beneficial in treating closely spaced or multiple intracranial targets. With integrated collision avoidance algorithms, HyperArc ensures safe delivery of complex non-coplanar arcs. HyperArc reduces planning and delivery time, allowing clinics to treat more patients with higher precision and confidence
In the afternoon, Dr. Binay Shrestha (Switzerland) joined online to present clinical workflows and plan evaluation protocols. He detailed standard operating procedures (SOPs) for various tumor sites treated with SBRT, including spinal metastases, lung nodules, and adrenal lesions.
Dr. K. Kanakavel (PTW, India) concluded the day with a hands-on demonstration of QA tools such as RUBY phantom for end-to-end testing and OCTAVIUS 4D for patient-specific dosimetric validation, explaining detector calibration, software use, and data interpretation. In the context of high-dose, high-precision radiotherapy like SRS, SRT, and SBRT, quality assurance (QA) is not just a regulatory formality—it is a clinical necessity. To maintain sub-millimeter accuracy and protect critical structures located near small targets, every component of the treatment chain must be meticulously validated. This is where advanced QA tools like RUBY and OCTAVIUS play a transformative role. Following the academic sessions on Day 2, the official inaugural ceremony took place. The event was attended by key dignitaries from BPKMCH, Bhaktapur Medical College, and SCMPCR, as well as the international faculty and workshop participants.
The ceremony began with a keynote address by Prof. Dr. Golam Abu Zakaria, Chairman of SCMPCR, who set the tone for the event with a powerful message on the importance of scientific workshops. Prof. Zakaria reaffirmed the belief in the transformative potential of education and innovation to shape a more sustainable and equitable world. The session continued with a compelling address by Prof. Dr. Hasin Anupama Azhari, CEO of SCMPCR, who shared the vision and mission of SCMPCR. Her remarks highlighted the organization’s commitment to building a stronger network of academic excellence, capacity- building, and resource-sharing in radiation oncology. She expressed optimism about the collective efforts of the region’s professionals in shaping the future of precision radiotherapy through unity and mutual growth. This formal opening ceremony marked the commencement of a meaningful journey into the realm of advanced radiotherapy techniques, setting a tone of inspiration and shared purpose for the days that followed.
Day 3: Hands-On Sessions in Contouring, QA, and Image Fusion: Day 3 emphasized skill-building through practical exercises. Applying theoretical concepts to real patient data ensures participants can confidently perform stereotactic procedures in clinical practice. Practical learning took center stage on Day 3, reinforcing theoretical knowledge through direct application. Participants were divided into Group A and Group B for parallel sessions.

Group A engaged in contouring exercises using real patient datasets under the guidance of Dr. Robert Semrau, Dr. S. Ghosh Laskar, and Varian experts. Tumor volumes and OARs were delineated, followed by peer-reviewed evaluations to highlight common contouring discrepancies. Group B worked with Mr. K. Kanakavel and Dr. Raju Srivastava on QA demonstrations, setting up the RUBY and OCTAVIUS systems for plan verification. They explored phantom positioning, dose delivery, and gamma analysis interpretation, including tips for mitigating measurement errors.
In the post-lunch session, both groups attended treatment plan evaluation sessions led by Dr. Binay Shrestha and Prof. Zakaria, who emphasized the use of Conformity Index (CI), Homogeneity Index (HI), Gradient Index (GI), and DVH (Dose-Volume Histogram) analysis in plan assessment.

Later, Group A participated in image fusion exercises, particularly 4DCT with PET-CT, while Group B focused on QA data interpretation, involving log file analysis and report generation.
Day 4: Evaluation and Certification: This day focused on consolidating knowledge through evaluation and charting a long-term vision for stereotactic radiotherapy in South Asia, emphasizing sustainability, collaboration, and academic growth.

Day 4 was dedicated to academic evaluation and strategic vision. An examination session was conducted byProf. Dr. Golam Zakaria, Dr. Raju Srivastava, and Prof. H.A. Azhari, assessing the participants’ understanding of stereotactic principles, workflows, QA, and radiobiology. The closing day featured a certificate distribution ceremony co-hosted by BPKMCH and SCMPCR. The workshop awarded each participant 38 Continuing Professional Development (CPD) points, officially recognized by professional regulatory authorities. This accreditation affirms the workshop’s academic rigor and its relevance to professional licensing and advancement. Participants expressed overwhelming satisfaction with the workshop’s structure, balance of theory and hands-on sessions, and the depth of international faculty interaction. Many noted that this training would directly influence how SRS, SRT, and SBRT are implemented at their home institutions. The event concluded with a festive group photo, exchange of tokens of appreciation, and a strong call for continued regional collaboration in building equitable, high-quality cancer treatment infrastructure.

Participant Reflection: Bridging Knowledge and Practice in Precision Radiotherapy.“Participating in the workshop was not merely an academic engagement—it was a transformative journey that expanded both my clinical insight and technical skill set”.
As a participant, I found the workshop at Bhaktapur Medical College to be exceptionally insightful and professionally enriching. The seamless integration of theoretical lectures with hands-on sessions allowed me to internalize complex concepts in SRS, SRT, and SBRT and apply them in practical scenarios. Each day brought a deeper appreciation for the intricacies of high-precision radiotherapy—from the radiobiological rationale and anatomical contouring to the implementation of advanced planning technologies like HyperArc and the robust quality assurance protocols using RUBY and OCTAVIUS systems. What stood out most was the opportunity to engage directly with global experts and peers from across South Asia. The discussions, case reviews, and interactive sessions not only deepened my technical knowledge but also fostered a spirit of collaboration and shared learning that I will carry forward in my clinical practice and academic journey.
I wholeheartedly encourage fellow medical physicists, radiation oncologists, and dosimetrists to participate in future SCMPCR workshops. These events are not only academically rigorous but also uniquely tailored to the regional challenges and opportunities in high-precision radiotherapy. Engaging with SCMPCR opens the door to a vibrant network of professionals committed to excellence, innovation, and cross-border collaboration in cancer care. Let us work together to build a stronger, more unified future for radiotherapy in South and Central Asia.
Sequential Sentence Classification in Structured Medical Abstracts: A Performance Comparison of Simple RNN and LSTM
Bushra Intakhab1* Savera Camran2
1Department of Physics, Florida Atlantic University, Boca Raton, FL 33431-0991, USA
2Department of Physics, Government Degree College Murad Memon, Karachi, Pakistan
Corresponding Author: bushraintakhab@gmail.com
Abstract
This study investigates the effectiveness of deep learning models SimpleRNN and Long Short-Term Memory (LSTM) for sequential sentence classification in structured medical abstracts. The task involves identifying the functional role of each sentence to facilitate evidence extraction in medical literature. Both models were trained and evaluated on a labeled dataset derived from scientific medical abstracts. Performance metrics indicate that the LSTM model significantly outperforms SimpleRNN, achieving a test accuracy of 75.36% and a macro-averaged F1-score of 0.6867, compared to 35.88% accuracy and 0.1720 F1-score for SimpleRNN. The LSTM model also demonstrated more balanced and accurate predictions across all sentence roles. These findings highlight the importance of using advanced recurrent architectures like LSTM for natural language processing tasks in the medical domain, supporting improved literature mining and automated knowledge extraction.
Introduction
With growing scientific data, the ability of machines to understand and process natural language text has become increasingly valuable especially in domains like medical physics, where practitioners rely heavily on the timely interpretation of scientific literature, clinical trial data, and treatment guidelines. One important task in this domain is sequential sentence classification, where each sentence in a structured document (e.g., a scientific abstract, clinical protocol, or radiotherapy guideline) is classified based on its role in the overall structure such as background, methods, results, or conclusions. In medical physics such automated classification can streamline literature review, identify relevant outcome data, and improve decision making by extracting evidence-based content more efficiently.
Recurrent Neural Networks (RNNs) have traditionally been used for sequence modeling due to their ability to retain context over sequences. However, Long Short-Term Memory (LSTM) networks, an advanced variant of RNNs, have demonstrated superior performance in tasks involving long-range dependencies, making them more suitable for interpreting structured medical texts.1 Dernoncourt and Lee introduced the PubMed 200k and 20k RCT datasets, which provide structured biomedical abstracts labeled at the sentence level. Their work demonstrated that sequential models like RNNs and LSTMs significantly outperform non-sequential baselines in identifying sentence roles. This dataset has become a benchmark for evaluating sentence classification in clinical and scientific domains.2 Mikolov et al. pioneered the use of Recurrent Neural Networks (RNNs) for language modeling, showing their effectiveness in capturing contextual dependencies. Their model marked a foundational shift toward deep learning in NLP tasks. However, the limitations of RNNs, particularly their struggle with long-term dependencies, led to the development of more advanced architectures like LSTM.3
This study explores and compares the effectiveness of RNN and LSTM architecture for the task of sequential sentence classification. By evaluating these models on labeled structured abstracts, we aim to determine which architecture better supports the extraction of scientific knowledge, with implications for automated literature mining.
Materials and Methods
The dataset used for this work consists of structured abstracts, where each sentence is labeled according to its role within the document such as background, methods, results, or conclusions. Sentences were first tokenized into individual words, transformed into numerical sequences using a tokenizer, and then padded to a consistent length to prepare them for model input. Two deep learning models were developed and compared: a Recurrent Neural Network (RNN) and a Long Short-Term Memory (LSTM) network. Both models were implemented using Python and Keras and were trained to classify the sentence roles based on word sequences. The training process involved splitting the dataset into training, validation, and test sets. Model performance was optimized using categorical cross-entropy loss and the Adam optimizer.
Model evaluation was conducted using standard classification metrics, including accuracy, F1-score, and a confusion matrix to assess performance across different sentence types. These methods enabled a comprehensive comparison of the two architectures in their ability to understand and structure scientific abstracts.
Results
Two deep learning models SimpleRNN and Long Short-Term Memory (LSTM) were implemented and evaluated for the task of sequential sentence classification on structured medical abstracts. The models were trained and tested using a labeled dataset where each sentence was assigned a role such as Background, Objective, Methods, Results, or Conclusions.
The SimpleRNN model achieved a test accuracy of 35.88% and a macro-averaged F1-score of 0.1720. In contrast, the LSTM model significantly outperformed SimpleRNN, achieving a test accuracy of 75.36% and a macro-average F1-score of 0.6867.
Metric | SimpleRNN | LSTM |
Accuracy | 35.88% | 75.36% |
F1-Score (Macro) | 0.1720 | 0.6867 |
Table 1. Performance comparison between SimpleRNN and LSTM models on the test datasetThe classification report also showed notable differences in class-wise performance:
Sentence Role | SimpleRNN F1 | LSTM F1 |
BACKGROUND | 0.00 | 0.51 |
OBJECTIVE | 0.03 | 0.59 |
CONCLUSIONS | 0.01 | 0.67 |
RESULTS | 0.27 | 0.81 |
METHODS | 0.55 | 0.85 |
Table 2:Class-wise F1-score comparison between SimpleRNN and LSTM models across different sentence roles in structured medical abstracts
The confusion matrices for both models further illustrate their classification behavior (Figure 1). The SimpleRNN model exhibits significant off-diagonal errors, particularly for the Background, Objective, and Conclusions classes, which are often misclassified as Methods or Results. In contrast, the LSTM model produces a confusion matrix with strong diagonal elements, indicating a higher degree of alignment between predicted and actual sentence roles.
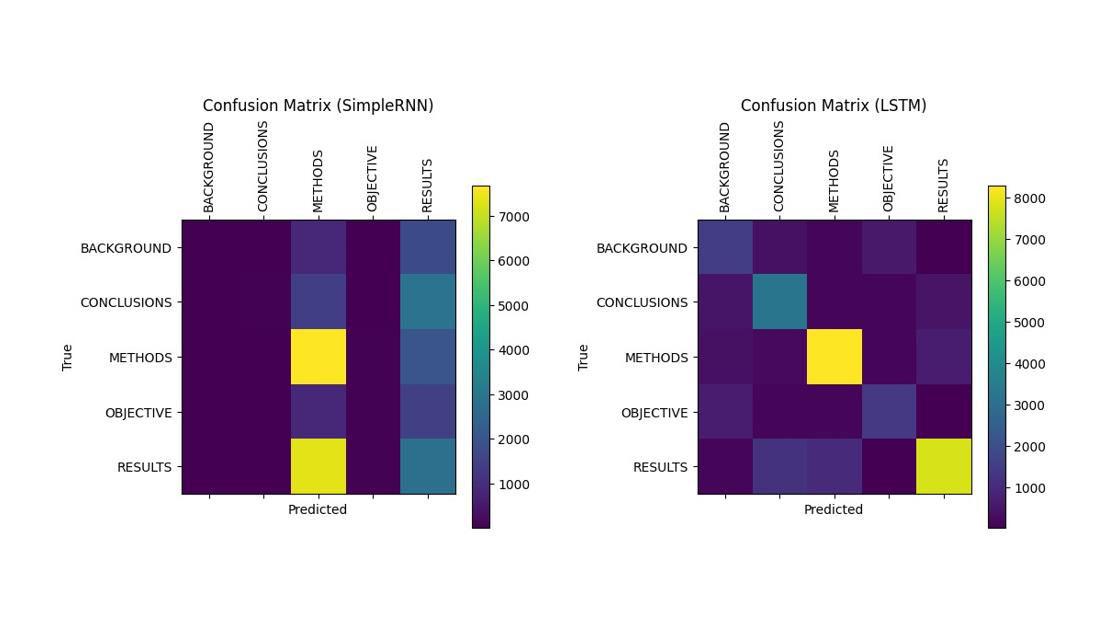 Figure 1:Confusion matrices for SimpleRNN (left) and LSTM (right) showing model predictions across five sentence roles in structured medical abstracts. LSTM exhibits stronger diagonal dominance, indicating more accurate classification
Figure 1:Confusion matrices for SimpleRNN (left) and LSTM (right) showing model predictions across five sentence roles in structured medical abstracts. LSTM exhibits stronger diagonal dominance, indicating more accurate classification
Discussion
The results clearly demonstrate that the LSTM model is more effective than SimpleRNN for classifying sentence roles in structured medical abstracts. This can be attributed to LSTM’s architectural advantage in capturing long-range dependencies and retaining contextual information across sequences a critical requirement in the interpretation of medical literature.
Simple RNN’s low performance, particularly in identifying BACKGROUND, CONCLUSIONS, and OBJECTIVE sentences, suggests that it struggles to distinguish among sentence roles when context from surrounding sentences is required. LSTM mitigates this limitation through its memory cells and gating mechanisms, which allow it to model complex patterns over longer textual sequences.
The substantial improvements observed in macro F1-score and overall accuracy suggest that LSTM not only classifies dominant classes like METHODS and RESULTS well but also maintains robustness in handling minority classes. This is particularly important in medical domains, where extracting conclusions or objectives from text can directly impact clinical decision-making and literature synthesis.
Overall, the findings confirm that for tasks involving sequential sentence classification in structured scientific texts, more advanced recurrent architectures like LSTM should be preferred over simpler RNNs. These insights contribute to ongoing efforts in automating evidence extraction and enhancing information retrieval in medical physics and related fields.
Conclusion
Overall, the LSTM model demonstrates a robust capacity for sequential sentence classification in medical physics literature, which can facilitate automated extraction of evidence-based content and support efficient literature reviews. These findings highlight the importance of choosing advanced sequential models for downstream applications in clinical natural language processing.
References:
- Hochreiter, , & Schmidhuber, J. (1997). Long short-term memory. Neural Computation, 9(8), 1735– 1780
- Dernoncourt, F., & Lee, J. Y. (2017). PubMed 200k RCT: a dataset for sequential sentence classification in medical abstracts. https://arxiv.org/abs/1710.06071
- Mikolov, , Karafiát, M., Burget, L., Cernocký, J., & Khudanpur, S. (2010). Recurrent neural network- based language model. In Proceedings of the 11th Annual Conference of the International Speech Communication Association (INTERSPEECH) (pp. 1045–1048).
BMPS celebrates International Medical Physics Week (IMPW) 2025
Md Akhtaruzzaman, PhD
Chief Medical Physicist, Evercare Hospital Chattogram
President, Bangladesh Medical Physics Society (BMPS)
The Bangladesh Medical Physics Society (BMPS) successfully organized a series of webinars from May 5 to May 9, 2025, to celebrate International Medical Physics Week (IMPW). This annual event aims to enhance global engagement in medical physics education and discussions. The webinar series featured four insightful lectures delivered by distinguished national and international experts, attracting approximately 450 participants from 42 countries.

The webinars were conducted virtually via Zoom, allowing professionals, students, and researchers in medical physics to participate freely. Each session focused on important topics relevant to clinical practices and advancements in the field.
The sessions include the following diverse medical physics topics:
- Understanding the Radiobiology of Brachytherapy (5th May)
- Geometric and Dosimetric Impact of Bladder and Rectal Filling on Pelvic Radiotherapy Quality Using 3DCRT, IMRT, and VMAT (6th May)
- Pediatric Radiotherapy in Resource-Limited Countries: Addressing Setup Errors, Anesthesia Challenges, Stochastic-Deterministic Risks, and Late Toxicity Using IGRT, IMRT, SGRT (8th May)
- Hypofractionation, Digital Image Formation in Medicine (9th May)
BMPS’s initiative in organizing these webinars fostered global collaboration, knowledge sharing, and professional development in medical physics. It provided a platform for medical physicists to discuss innovations, challenges, and emerging techniques in radiation therapy, imaging, and clinical applications. The IMPW 2025 webinar series was a resounding success, demonstrating BMPS’s commitment to promoting medical physics education worldwide. The engagement of considerable participants from across the world highlights the increasing interest in the field and the importance of continued efforts to advance medical physics research and practice.
A deep dive into the challenges, advancements and future directions in Medical Physics: Insights for South Asia
Prof. Dr. Mary Joan
Radiological Safety Officer and Vice Principal Academics (IAHS) at the Christian Medical College and Hospital, Ludhiana, India
The South Asia Centre for Medical Physics and Cancer Research (SCMPCR) is committed to enhancing the fields of medical physics and cancer research across South Asia, with the ultimate goal of improving patient care and advancing global health. Through a range of comprehensive teaching and training programs, SCMPCR actively addresses the unique challenges faced by medical physicists in the region. What began as a foundational vision by pioneering leaders has evolved into a period of dynamic growth, driven by strategic collaborations and partnerships. Building on these early efforts, SCMPCR has accelerated progress with impactful and innovative training initiatives. The SCMPCR newsletter is another initiative which celebrates the accomplishments of medical physicists and promotes active medical physics endeavors, fostering sustainable partnerships and cooperative efforts throughout South Asia.
In this issue, we delve into the challenges, advancements, and future directions in Medical Physics: Insights for South Asia,” featuring an interview with Dr. Frank Hensley. Join us as Dr. Hensley shares his expert perspectives on the evolving landscape of medical physics, exploring both the advances that are transforming the field and the regional challenges that remain. Here is a snippet of the chat with Dr Hensley by Dr. Mary Joan regarding his contributions and involvement in establishing SCMPCR activities.

Dr. Frank Hensley studied physics and mathematics in Heidelberg where he majored in nuclear physics and astrophysics. He entered medical physics in 1979 at Essen University Hospital as postdoc in a project on
radiotherapy with neutrons. After this term he worked in radiotherapy and nuclear medicine at several hospitals in Germany. He returned to academia at Heidelberg University Hospital in 1990 where apart from general radiotherapy he specialized in Brachytherapy and treatment with electrons, including intra operative radiotherapy, Total Skin Electron Therapy and Total Body Irradiation. During his career he had the opportunity to gain experience in teaching students from emerging countries including Mongolia, Turkey, Chile and
Bangladesh. After retirement from the clinical in 2014, he continues working in standardization of radiotherapy and on basic topics in dosimetry. He is member of the German Society for Medical Physics DGMP, the German Physical Society DPG, the American Association of Physicists in Medicine AAPM and the German and European Societies for Radiation Oncology DEGRO and ESTRO.
MJ: Glad to have this opportunity to hear you. Would you please share your early experiences and what prompted you to venture into medical physics as a career?
FH: Originally I had not planned to end up in medical physics. I majored and obtained my PhD in nuclear physics. But by the time I had finished my thesis, physics jobs had become rare, both at the university and in nuclear engineering. So I joined a project in radiation therapy with neutrons at the university hospital in Essen. As circumstances play, neutron therapy was abandoned about a year after I had started, due to unacceptable complications in the patients. So I looked into conventional radiation therapy at the neighbouring radiotherapy department and found that there was a lot to do. Those were still the early days in modern radiotherapy, planning with computers and very scarcely with CT information was just beginning. And the situation for medical physicists was not unsimilar to that in parts of South Asia today: physicists were scarce and not very well accepted in medicine. But I learned that there were always a few MDs around who were eager to work together with physicists – to get things going and to make use of all the new developments. And I learned that it was fun to work in an interdisciplinary team where everybody put in his or her share of expertise to improve therapy – for the patients. So I stayed in the field, ventured through several hospitals until I ended back at a University Hospital in Heidelberg. And all along, I always found MDs and RTTs –and physicists – who were a lot of fun to work with. And I learned that medical physicists have an extremely important job, implementing new technology into medicine and then being responsible for organizing and maintaining its safe use. And there is a lot of interesting physics in the job, too.
MJ: what are the professional differences in being a medical physicist in Germany compared to South Asia? Please elaborate on the important aspects?
FH: I guess the obvious difference is in the availability of resources. In an industrial country like Germany all the new technical developments are immediately available and desired by both physicians and patients. But that does not mean that they are immediately present in your work. You need to clarify together with the MDs what can be used and afforded, and what fits into the
procedures applied at your hospital. Then you must analyse how within these constraints the new techniques can be adjusted safely to workflows at your institution, reflecting the present state of science. You must design workflows that comply with the active regulations, and develop commissioning and quality assurance procedures adapted to the planned methods. So actually there are large similarities and our work is mainly happening at a different stage of technical development: while in many places in South Asia you must first convince
the medical and political society of the priority of technological medicine, in an industrial company you must convince the people who finance and direct your work of the priority of a certain new development. And following that you have to do largely the same kind of work.

MJ: You have personally nurtured many collaborations for SCMPCR. Please enlighten us on the early status and challenges?
FH: Actually the Bangladesh-German collaboration had begun several years before I entered, when Abu Zakaria gathered a group of medical physicists from Germany who travelled to Bangladesh and held seminars at universities and hospitals to inform the scientific and medical society of the need for physics in modern radiation medicine. This led to the installation of the first training program in clinical medical physics at Gono University and even to the foundation of professional association of physicists interested in the development of medical physics, the BMPA. I myself got involved in the project when some of the first students from Gono University came to Germany to perform experiments for their graduation theses. That was when I got to know a number of the people who are now active in medical physics in Bangladesh: Hasin Anupama Azhari, who worked on her thesis at my department at Heidelberg University Hospital, Md. Akhtaruzzaman, Anwarul Islam, Masud Rana, Sinha Khalid, Harun Rashid and more who all worked at the German Cancer Research Center in Heidelberg.

In the following years we were lucky to achieve sponsoring by the German Academic Exchange Service DAAD who supported the collaboration between Heidelberg and Gono universities. With these funds we could finance equipment, scientific exchange and travel. In this program we could invite a substantial number of medical physics students for study years at Heidelberg University’s Medical Facilities in Mannheim. In this period fell the foundation of SCMPCR which in its beginning phase could profit from equipment funded by the project for teaching purposes and whom we helped recruiting speakers, and also with travel grants. Many of the young students that visited us in Germany now belong to the leaders in the field of medical physics in Bangladesh and we are all very proud of the excellent work they are doing.
Regretfully, the work of two important early foundations is momentarily somewhat disturbed. The university training course in medical physics has been interrupted, and a new course must be established at a new university. This is momentarily well under way in negotiations, and we hope it will be soon continued. Second, some misunderstandings have arisen among the physicists involved in medicine which has led to the separation of the professional societies into BMPS who represent the interests of clinical medical physics and BMPA who represent physicists working on medical topics at classical universities. It is paramount that these two groups of physicists recognize the importance of working together: medical physics needs the basic education and university physics must support the extended pathway to medical applications required by society. The competitive situation today blocks many important developments when government and administration hear only one group’s argumentation or international agencies like IAEA are allowed to support only one national society.
MJ: How do you look at the present professional scenario for medical physicists in South Asia?
FH: The professional perspective of medical physics is excellent, or at least should be so. South Asia includes many countries with huge populations and therefore – regretfully – also large numbers of patients in need of radiation medicine. For this, many physicists are needed, and also many radiotherapy and radiation medicine institutions must be founded to treat the large number of patients needing this service. Also universities should acknowledge this need and recognize the large number of valuable positions this can yield for their graduates: positions in radiation therapy and diagnostics, in nuclear medicine, and also in the biomedical engineering field, in the development of instrumentation, and also in sales and maintenance. The foundation of all of this is a sound basic scientific education which schools and universities must provide. The specialized training in clinical medical physics is then a task which universities cannot easily fulfil. Training must happen with real, newest-generation medical equipment and with real patient cases. For this specialized training, teaching institutions are needed which collaborate closely with hospitals, and continuing education for professionals must be organized. And for the institutions providing this training, qualified teachers are needed which again opens a large number of positions and a large requirement of training. And all of these positions and institutions should be generously embursed because they provide an important service to society.
MJ: Kindly share your most memorable experiences in your collaborations?
FH: The great experience is to see how the people who started off as students many years ago have now matured to be among the leaders in their profession. And it is especially exciting to see how this is happening in a completely different cultural setting. Challenges in South Asia are different and some are probably larger than in Europe. Basically, we all have the same interest to be of help in the battle for our patient’s health. But in the different lifestyle and even life philosophy in South Asia (and other parts of the world) it is an additional challenge to to combine the need of a very strict and exact analytical perspective in modern science to the rich and colorful, but technologically less experienced cultures and life styles in your countries. And at the same time one must acknowledge that developing all the technology and the political culture behind technology also in the industrialized countries, was (and still is) a struggle against many aberrations that also occur, and can lead to social injustice, or as we are presently observing, to the destruction of our planet. Working in technological development you need to deal with all of these issues. I am optimistic that South Asia can succeed in this struggle, given the overwhelming hospitality and devotion of the people here. But on the other side it is disturbing to see how large parts of society are neglected and excluded from the benefits of technical development. So, I believe it would be a wonderful experience to see our partners integrating solid scientific work into the advancement of unique cultures, adjusted to their countries and heritage, but at the same time working towards social balance and equal opportunities.

MJ: What are the future prospects medical physicists in South Asia needs to be prepared for?
FH: Medicine is making large advancements in many fields – beginning with the omnipresent use of artificial intelligence, but also in the more basic fields of computerization, automation and robotics. This is happening in all medical disciplines, not only in radiology. Handling and mining big data will achieve a major role in understanding causes and cures of diseases but also in organizing healthcare. We are presently seeing this development in our field in radiomics and the development of image guided and automatically adapted
radiotherapy. Physics is the scientific basis of all of this, and specialized physicists are needed in the development and engineering in advanced applications in almost all fields of medicine. Experimental physics develops and exploits all of these techniques for its own scientific use, so it is an ideal training ground from which technical methods can be translated into many other applications. It is therefore helpful when young physicists have broad interests and also look into in other scientific fields, medicine is only one of them. And then they need to keep updated during their entire professional life by continuing education.
A completely different area in which medical physicists should take a leading role in is the development of general organizational issues in the topics related to their work. This begins with the development of the regulations needed to ensure quality and safety in the technical field, as well as regulations for preventive maintenance to ensure sustainable and long-living operation of the expensive technical facilities. Such a framework of regulations should be based on the collaboration of all medical professions but also the universities and teaching institutions and it should be integrated into a forward-looking development of general healthcare for all of the society.
MJ: What would be your advice to young medical physicists of South Asia for career development?
FH: Start off with a good physics and mathematics background. You need math not only to calculate things, but to logically analyse how things work and what causes malfunctions. That is something you spend a lot of time with as medical physicist. And then, stay curious and keep updated on new developments. Implementing new methods is a core part of medical physics work. And do this in collaboration with Rad Oncs and RTTs. – For this you need a solid understanding of the medical background so you can collaborate at eye-level with the MDs, and mutually understand why and what you need to do.
Keep involved and informed in the ongoing science in physics, but also in medicine and the other fields. Hospital work leaves only a small amount of time for scientific work but you need to use scientific methods to understand new techniques and to test and adapt them to the specific workflows in your own hospital, and then to develop individually adjusted quality assurance. So, organize some work time for measurements and developments. Convince your superiors that a thorough understanding of new developments and how to correctly apply them is essential to maintain the desired standards.
And then network and share your expertise, and learn to work in large teams. Organize professional exchange and training visits, for yourself, but also provide this to others at your own department. It is always advisable to teach – other physicists, RTTs, MDs, and also the general public. A rewarding fact is that the teacher himself always learns the most.
MJ: SCMPCR is planning to venture into publishing a medical physics journal in the coming years. What ground works needs to be done before that?
FH: Well, actually I think we should be careful in expanding the number of publications. Too many publications are typically connected with a loss in quality and more difficulty for readers to distinguish between important and unimportant papers, and, simply spoken, it requires more reading effort. We presently already have around 15 journals publishing medical physics content. So if one wants to start an additional journal, it should be dedicated to some content that is not yet sufficiently represented. On the other side, practically oriented journals tailored to the specific needs of a certain group can be helpful. I believe a starting point could be such an application-oriented journal in which physicists can share practical experiences, in technical but also in organizational affairs; a journal where you can find information on job and training opportunities, organize mutual help in every day work, and discuss common unified ways of advocating medical physics needs and interests This could be specially dedicated to the situation in South Asia. To share scientific content, I would rather suggest submitting high quality manuscripts to the existing international
journals (being accepted there is also a good quality control) and encourage strengthening larger local journals like the Indian Journal of Medical Physics.
Such a practical journal could be published electronically, similar to the SCNPCR newsletter and it should be open access. That would also make it interesting for vendors to disseminate commercial information and advertisement.
MJ: What are your visions for SCMPCR and where do we need to focus more?
FH: First of all I would like to congratulate SCMPCR for the great job they are already doing. I would wish the center continues providing first class information to the large numbers of physicists they are now already addressing. Using the possibilities of virtual meetings and e-learning, SCMPCR is now reaching an audience across entire South Asia and into Africa in a quality that even causes European listeners to tune in. I am also happy about SCMPCR’s activities in strengthening public health. Using its resources to organize vaccination campaigns and cancer awareness education underlines SCMPCR’s importance as a valuable contributor to the development of health care for all. And of course, the future still requires large efforts in basic medical physics training. SCMPCR should play an active role in the development of a medical physics training program customized to the local needs. In this field there is a large potential in active collaboration: SCMPCR should collaborate with the training universities and hospitals but also with the general universities providing basic science education. Teachers and students could be exchanged and attend lectures at several cooperating universities. In this way missing expertise could be completed and information shared. Curricula should be adjusted to another so bachelors entering medical physics have a solid foundation. SCMPCR should continue collaborating with MDs in seminars and training courses so that physics education keeps close pace with the medical applications and vice versa. SCMPCR should serve as a hub for communication and networking between physicists and also with MDs, and it should be a bridge to international institutions like IAEA ant the international physics organizations. One of the early goals was establishing a virtual library including access to electronic media and journals. However this is an expensive project, so it requires support by external financers, mainly the state, but also the vendors who are also interested and rely on working with well- educated users could contribute.
And finally, SCMPCR should take an active role in the development of therapy but also in healthcare and the development of regulations as I have already mentioned earlier. This is needed to provide the safe use and maintenance of medical equipment and methods, to define the educational requirements, and the requirement and availability of expert staff. All this helps achieving acceptance in the medical world, where physicists should work together at eye-level with the MDs for the patient’s well-being. And to earn this acceptance we must convince the medical world by the quality of our work.
So, there is plenty to do in the future – let’s get into it!
MJ: As we wrap up this insightful conversation with Dr. Frank Hensley, it’s clear that the journey of medical physics in South Asia is at a critical juncture—rich with both challenges and immense potential. We extend our heartfelt thanks to Dr. Frank Hensley for sharing his valuable insights, experiences, and vision for the future of medical physics. His perspectives have not only shed light on the current landscape but also inspired a proactive approach to the development of the field in South Asia. We deeply appreciate his time and thoughtful contributions to this important dialogue. His call to action highlights the essential role organizations like SCMPCR must play, not only in advancing therapeutic practices but also in shaping healthcare policy, regulation, and education. By prioritizing quality, collaboration, and a shared commitment to patient care, medical physicists can secure their rightful place alongside clinicians. The path ahead is demanding, but also inspiring—let’s rise to the challenge together.
Prof. Dr. Mary Joan serves as the Radiological Safety Officer and Vice Principal Academics (IAHS) at the Christian Medical College and Hospital, Ludhiana, India. She is the Chair of the Professional Relations Committee of AFOMP, a member of the Science Committee of IOMP, and part of the Executive Committee of AMPI-NC. She also holds the position of Co-Editor-in- Chief of the SCMPCR Newsletter.
Dosimetric Feasibility of Applying the Fast Forward Trial Protocol for Breast Radiotherapy Using a Co-60 Machine in Resource-Limited Settings
Buddhika Srimal Sesath
Medical Physicist, Teaching Hospital, Badulla, Sri Lanka
In a significant development for global radiation oncology, a study conducted at the Teaching Hospital, Badulla, Sri Lanka has demonstrated the potential of delivering the Fast Forward breast radiotherapy protocol using cobalt-60 (Co-60) machines. Originally designed for advanced linear accelerators, the Fast Forward protocol’s successful adaptation to Co-60 systems could provide a breakthrough in cancer treatment for low- resource countries.
This research, presented at ICARO-4 (International Conference on Advances in Radiation Oncology), evaluates the dosimetric feasibility of implementing the 26 Gy in 5 fractions Fast Forward regimen on Co-60 equipment and compares it with the conventional 40 Gy in 15 fractions regimen in right-sided breast cancer patients. The study was led by Oncologist Dr. P.K.D.P. Alahakoon (MD) and Medical Physicists Buddhika Srimal Sesath (MSc) and J.H.J.K. De Silva (MSc).
The Fast Forward trial, developed for modern linear accelerators (LINACs), demonstrated clinical safety and efficacy in reducing treatment time for breast cancer patients by using larger dose fractions over a shorter schedule. However, applying this regimen on Co-60 teletherapy machines, still widely used in many low- and middle-income countries, presents unique challenges due to their physical limitations, such as lower photon energy and broader penumbra.
Hypofractionated radiotherapy offers significant advantages: shorter treatment duration, increased patient throughput, and potentially improved patient compliance—critical benefits for overloaded public health systems.
This study explored whether these modern protocols could be adapted for legacy equipment without compromising treatment quality or patient safety. The primary objective of this study was to assess the dosimetric feasibility of delivering the Fast Forward breast radiotherapy protocol—administering 26 Gy in 5 fractions—using a cobalt-60 (Co-60) machine, which is more commonly available in resource-limited settings. A secondary goal was to compare the outcomes of this hypofractionated regimen with the conventional 40 Gy in 15 fractions treatment. The study focused on evaluating critical treatment planning parameters such as planning target volume (PTV) coverage, radiation doses to the heart and lungs, and dose homogeneity. Special attention was given to analyzing differences in dosimetric outcomes between patients who underwent mastectomy (MA) and those who received wide local excision (WLE), in order to determine the protocol’s suitability across diverse clinical scenarios.
The study included a total of 74 patients diagnosed with right-sided breast cancer, comprising 39 individuals who underwent Modified Radical MA and 35 who received WLE All patients were planned using the PCRT- 30 protocol for 3D-Conformal Radiotherapy (3D-CRT) delivered with a cobalt-60 (Co-60) unit. In accordance with the Fast Forward protocol guidelines, the CTV, PTV, and OARs were carefully delineated. Treatment planning involved the use of two tangential glancing beams with wedges, a widely accepted technique to effectively cover the breast or chest wall. Particular attention was given to ensuring uniform PTV coverage and optimizing dose homogeneity, while simultaneously minimizing radiation exposure to critical organs such as the heart and lungs.
DOSE PER FRACTION (GY) | KEEP 30% OF DOSE TO < 15% OF IPSILATERAL LUNG VOLUME | KEEP 25% OF DOSE TO < 5% OF HEART VOLUME | KEEP 5% OF DOSE TO < 30% OF HEART VOLUME |
2.67 | 12.0 Gy | 10.0 Gy | 2.0 Gy |
5.2 | 8.0 Gy | 7.0 Gy | 1.5 Gy |
Table 1: Dose Constraints for OARs
The use of Co-60 presented several technical challenges in the context of breast radiotherapy. One of the primary limitations was its lower photon energy compared to LINACs, which reduced beam penetration and increased scatter, thereby affecting overall dose distribution. Additionally, Co-60 systems produce a larger penumbra, resulting in less precise dose conformity at the field edges and making it more difficult to spare adjacent OARs, such as the heart and lungs. These factors necessitated increased planning efforts to reduce hot spots and ensure a consistent and uniform distribution across the PTV, while still maintaining treatment effectiveness and safety.
The results of the study highlighted several key findings related to dose homogeneity and OAR sparing. In terms of dose homogeneity, WLE plans demonstrated superior performance, with a lower average HI of 0.51 compared to 0.68 in modified radical MA plans, indicating more uniform dose distribution in WLE cases. Regarding heart dose, MA plans consistently resulted in lower mean heart doses across both the 26 Gy and 40 Gy regimens. However, in both MA and WLE plans, a relatively higher percentage of heart volume received 5% of the prescribed dose, although less than 5% of the heart volume received 25% of the total dose in either treatment regimen, remaining within acceptable constraints. Lung dose metrics also showed promising results, with the volumes of lung receiving 30% of the dose being similar in both dose schedules. The differences in lung dose between MA and WLE groups were minimal, underscoring the ability of Co-60 systems to adequately spare lung tissue with careful treatment planning.
The study demonstrates that WLE plans provide superior dose homogeneity, which may contribute to better long-term cosmetic outcomes and a reduced risk of radiation-induced complications. Conversely, modified radical MA plans, although less homogeneous, consistently result in lower mean heart doses—likely due to the increased distance between the heart and chest wall in post-mastectomy patients. Importantly, both MA and WLE plans successfully met established dose constraints for the heart and lungs under both the Fast Forward protocol and the standard regimen. These results strongly support the clinical feasibility of delivering the Fast Forward protocol using Co-60 machines for breast radiotherapy, making it a viable treatment option in resource-limited settings.
The study was inspired by the outcomes of the UK FAST and FAST- Forward trials and demonstrates how global radiotherapy guidelines can be adapted for low-resource environments. It paves the way for more equitable access to evidence-based cancer care worldwide. The research team acknowledges the foundational work of the UK Standardization of Breast Radiotherapy (START) trials.
Smarter, Faster, Safer: The Rise of Fully Automated Radiotherapy Planning
Ijaj Ahamed Rifat1, Md. Mokhlesur Rahman1/em>
1Department of Medical Physics and Biomedical Engineering, Gono Bishwabidyalay (University).
Introduction: A New Era in Cancer Treatment
Imagine if creating a radiation treatment plan for a cancer patient could be done with just one click. No long hours of manual work, no back-and-forth between different steps — just fast, efficient, and reliable results. This might sound like science fiction, but thanks to a groundbreaking system developed by a research team at the University of Alabama at Birmingham, it is quickly becoming a science fact.
Their new method for fully automated treatment planning recently outperformed dozens of other international teams in the 2023 Auto-RTP Challenge, a global competition focused on improving how we plan radiotherapy for cancer patients. Their success shows us that the future of cancer care could be faster, more precise, and more consistent than ever before.
What is the problem?
Radiotherapy is a common treatment for cancer that uses carefully targeted radiation beams to kill cancer cells. But before any treatment can happen, doctors need to create a detailed plan — a sort of “radiation map” to make sure the beams hit the tumor and avoid healthy organs. This process is complex, time-consuming, and depends heavily on expert judgment. Small mistakes or delays can affect treatment outcomes.
So, what if we could automate that process — and still make it just as good, or even better?
The Team’s Mission: A Smarter Way to Plan
The team’s goal was to develop a fully automated radiotherapy treatment planning system that could work on its own — from start to finish — with minimal human input. To test their system, they took part in the Auto- RTP Challenge, where participants were asked to create treatment plans for prostate cancer patients with the participants CT scans.
This challenge was tough. The plans had to follow unfamiliar guidelines and different dose levels than what the team usually used in their clinic. Yet, the team’s system adapted easily — and it won first place in all three phases of the competition.
How Does the System Work?
Think of the system like a self-driving car — but for treatment planning. It works in two major stages:
- Auto-contouring: First, it uses artificial intelligence to identify and label important parts of the body on a CT scan. These include the tumor and organs like the bladder and rectum, which need to be protected from too much radiation.
- Auto-planning: Next, it creates the best possible radiation plan based on those It decides how many radiation beams to use, where to aim them, and how strong each beam should be.
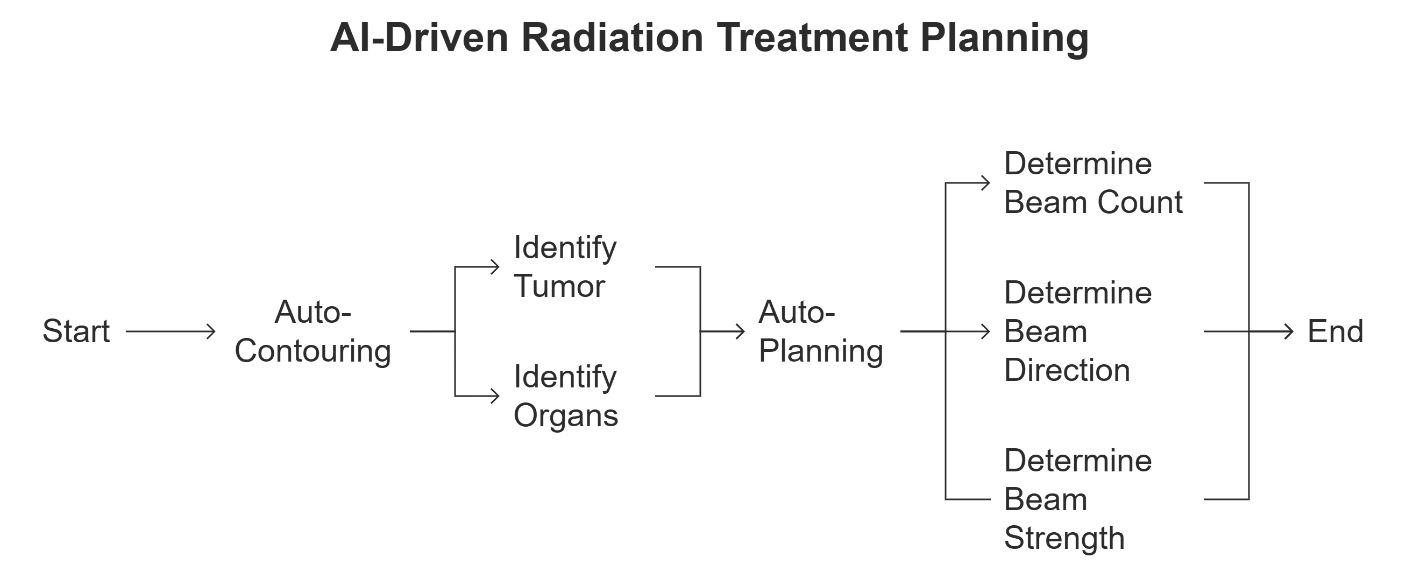
To do this, the system uses three powerful tools:
- Knowledge-Based Planning (RapidPlan): It learns from past treatment data to guide current
- Multicriteria Optimization (MCO): It balances trade-offs between different goals — like hitting the tumor hard while avoiding healthy tissue.
- Plan Scorecards: These are like report cards that grade the quality of each plan, ensuring high standards are met every time.
Why Does This Matter?
There are a few big reasons this research is exciting:
- Speed: The system created full treatment plans in under 41 minutes on average — a process that usually takes hours or even days.
- Consistency: Unlike humans, the system does not get tired or make mistakes. It can produce high- quality plans again and again.
- Adaptability: Even when asked to follow unfamiliar rules and prescriptions, the system performed well — a sign that it could be used in clinics around the world, even those with different treatment
- Reduced Workload: This can significantly ease the burden on busy clinical staff, giving them more time to focus on patients.
Results That Speak for Themselves
The team tested different combinations of planning strategies and found that combining Rapid Plan with MCO and scorecards gave the best results. This combination scored the highest on both their own data and in the challenge.
In one part of the challenge, called the “Plan Only” phase, their best strategy achieved an average score of 90 out of 100 — topping the leaderboard. This score reflects how well the treatment protected healthy organs while effectively targeting the cancer.
Looking Ahead: What is Next?
While the results are promising, there is still work to do. The current system relies on mathematical scores to judge plan quality, but doctors also need to visually inspect plans to make sure everything looks safe and effective. Future studies will focus on how these automated plans perform in real clinical settings, where human overview remains essential.
Still, this research marks a major step forward. It proves that with the right combination of AI tools, we can create safe, high-quality radiotherapy plans — automatically.
Conclusion: Towards a Smarter Future in Cancer Care
This study is more than a technical achievement. It is a glimpse into the future of cancer treatment — where powerful algorithms support medical teams, speed up care, and ensure every patient receives the best possible plan.
As automated systems continue to improve, they could help expand access to top-quality cancer care, especially in areas with limited medical staff. In short, this research is helping turn a time-consuming, expert- heavy task into a streamlined, smart process that brings better outcomes to more people.
Reference:
- Thompson, F., Valdes, G., Fuller, C. D., et al. (2018). Artificial intelligence in radiation oncology: A specialty-wide disruptive transformation? Radiotherapy and Oncology, 129, 421–426. https://doi.org/10.1016/j.radonc.2018.05.030
- Callens, D., Malone, C., Carver, A., et al. (2024). Is full-automation in radiotherapy treatment planning ready for take off? Radiotherapy and Oncology, 201, 110546. https://doi.org/10.1016/j.radonc.2024.110546
- Babier, A., Zhang, B., Mahmood, R., et al. (2021). OpenKBP: The open-access knowledge-based planning grand challenge and Medical Physics, 48(11), 5549–5561. https://doi.org/10.1002/mp.14845
- Rayn, K., Clark, R., Magliari, A., et al. (2023). Scorecards: Quantifying dosimetric plan quality in pancreatic ductal adenocarcinoma stereotactic body radiation Advances in Radiation Oncology, 8, 101295. https://doi.org/10.1016/j.adro.2023.101295
- Jayarathna, S., Shen, X., Chen, R. C., Li, H. H., & Guida, K. (2023). The effect of integrating knowledge-based planning with multicriteria optimization in treatment planning for prostate Journal of Applied Clinical Medical Physics, 24(7), e13940. https://doi.org/10.1002/acm2.13940
The GCB Summer School of Medical Physics at Hokkaido University: A Unique Opportunity for Faculty, Researchers, and Students
Md. Mokhlesur Rahman¹, Md. Abdullah¹
¹Department of Medical Physics and Biomedical Engineering, Gono Bishwabidyalay (University), Savar, Dhaka
Hokkaido University in Sapporo, Japan, annually hosts a prestigious and internationally acclaimed summer school tailored for emerging researchers and students in biomedical science and medical physics. From August 18 to 22, 2025, the Global Center for Biomedical Science and Engineering (GCB)—in collaboration with the Stanford University School of Medicine—will conduct two parallel summer schools: Medical Physics and Molecular Biomedical Science and Diagnosis.
Participants will receive advanced theoretical and hands-on training in a range of cutting-edge topics, including Metabolic PET imaging in the context of cancer ferroptosis, FLASH – A Paradigm Shift in Cancer Radiotherapy, Immuno-PET in Oncology, Overview of radiation therapy (Therapeutic Window in New Era), Overview of Diagnostic Imaging and Medical AI, Interaction of therapeutic radiations with matter, Boron Neutron Capture Therapy and its measurement device development, Introduction to Geant4 for particle therapy, Introduction to proton therapy systems, Proton therapy QA, Deep learning for advanced radiation therapy, Role of radiotherapy in cancer treatment, Clinical application of proton beam therapy, Dose calculation algorithms for spot scanning proton therapy, Hands-on Practical Training: Treatment Planning, Introduction to AI, Real-time image-guided radiation therapy, AI for MR-guided adaptive radiation therapy, Radiomics, Theranostics in Nuclear Medicine, Particle beam therapy equipment: towards ultra-high dose rate irradiation, and Clinical and biological evaluation metrics and biomarker in-silico in radiation oncology.
A highlight of this academic event is the 12th GCB Biomedical Science and Engineering Symposium, jointly organized by Hokkaido University and Stanford University. The symposium provides a global platform for participants to present and discuss innovations in biomedical science and medical physics with leading experts and fellow researchers from around the world. Md. Mokhlesur Rahman, Assistant Professor at Gono Bishwabidyalay, commented, “International programs like this serve as a gateway for Bangladeshi medical physics students to access advanced research environments and higher education opportunities. It is a rare and valuable platform for both academic enrichment and international collaboration.”
In 2025, Md. Mokhlesur Rahman, along with students—Md. Abdullah and Md. Rakib Hosen—will proudly represent Gono Bishwabidyalay as fellowship awardees at the GCB Summer School of Medical Physics. Their selection underscores the growing recognition of Bangladesh’s talent in the global medical physics community.
This initiative is especially impactful for graduate students and early-career researchers, helping them build global connections and expand their academic horizons.
No registration fee is required, and all selected participants will receive an official certificate from Hokkaido University.
For further details and application, visit: https://gcb.med.hokudai.ac.jp
The Dual Identity of Medical Physicists: Balancing Clinical Service and Research
Shriram Rajurkar
Assistant Professor, Department of Medical Physics, CIR, D. Y. Patil Education Society, Kolhapur, India.
Medical physicists are vital members of modern healthcare teams, operating at the interface between science and clinical practice. They not only ensure safe and accurate delivery of radiation therapy and diagnostic imaging but also push the boundaries of technological innovation through research and development. However, the dual nature of this profession straddling clinical responsibilities and research aspirations poses challenges that institutions, professionals, and academic programs must address. This article explores the evolving role of the medical physicist, one mended between clinical and research commitments, and practical strategies for achieving a sustainable balance.
Clinical Service: The Unseen Backbone of Radiotherapy
In routine clinical settings, medical physicists are indispensable. Their primary duties include commissioning and calibrating radiation therapy equipment, performing patient specific quality assurance for radiation treatments, ensuring compliance with radiation safety regulations, routine treatment planning among many other works. These tasks are often time sensitive and demand meticulous attention. In radiotherapy departments, a physicist’s role is crucial in ensuring the correct dose is delivered to the right location with high accuracy since deviations in a patient’s plan or machine performance can lead to underdosing the tumor or over exposing healthy tissues. In high volume hospitals, especially in low- and middle-income countries, the clinical workload is always intense. A small team of physicists may be responsible for hundreds of patients per week, leaving little bandwidth for academic or research activities. This workload, while essential to patient care, can limit innovation if not managed effectively.
The Research Mandate: Driving the Future of Medical Physics
On the research front, medical physicists contribute to advancements in radiation oncology, imaging technology, dosimetry, artificial intelligence applications, and more. Research is the engine that drives improvement in treatment efficacy, patient safety, and workflow efficacy and efficiency. Medical physics is not static; each advancement in treatment hardware, therapy software, or computing power introduces new questions that physicists are uniquely qualified to answer. However, this progress depends on time, funding, and institutional support resources often scarce in busy clinical environments.
The Academic Medical Physicist: Bridging Two Worlds
Academic medical physicists play a unique and essential role. Positioned in universities or teaching hospitals, they are typically involved in:
- Teaching graduate students and residents
- Supervising clinical training programs
- Conducting original research
- Collaborating with industry and clinical partners
These professionals are often the linchpin connecting clinical insights with theoretical innovation. For example, a clinical problem such as image drift in MRI-guided radiotherapy can be studied in a lab, modelled mathematically, and solved through interdisciplinary research. However, academic physicists also face time pressure from teaching loads, grant writing, and administrative duties. Without structured support and funding, their potential impact on both patient care and scientific advancement may be underutilized.
The Challenge: Time, Workload, and Institutional Culture
One of the greatest obstacles to balancing clinical and research responsibilities is time allocation. In many hospitals, the emphasis is almost exclusively on immediate clinical service, with research viewed as an optional extra. This creates a culture where research may be deprioritized, even though it is essential for long term clinical improvement. This imbalance can lead to “a missed opportunity to exploit the full potential of medical physicists.” It called for formal recognition of research as an integral part of a physicist’s role, with corresponding adjustments in workload and performance metrics.
Strategies for Balance: Recommendations and Solutions
1 Protected Research Time
Hospitals and cancer centers should allocate defined blocks of time for research. Whether one day per week or 20% of total workload, this “protected time” allows physicists to engage in scientific inquiry without clinical pressure.
2. Dual Track Career Models
Institutions can offer parallel career paths, one with a clinical emphasis and another focused on research. This allows professionals to pursue their strengths while contributing meaningfully to the field.
3. Collaborative Research Models
Physicists can co-lead clinical trials or work with radiation oncologists, radiologists, and data scientists to address practical clinical challenges. Embedding research into clinical operations allows for real-world impact and greater feasibility.
4. Investment in Staff and Resources
In high workload centers, hiring additional staff or delegating non-specialist tasks (e.g., administrative reporting) can free up physicists for innovation. Using automation and AI for QA can also reduce repetitive burdens.
5. Academic Clinical Partnerships
Stronger ties between universities and hospitals can provide access to research infrastructure (e.g., labs, computing clusters) and students, creating an ecosystem where ideas move fluidly from bench to bedside.
The Way Forward: Recognizing Value Beyond Service
Medical physicists are more than simple clinical occupational workers, they are innovators, educators, and leaders in the fight against cancer. To fully harness their potential, both clinical institutions and academic centers must invest in integrated roles that value both clinical service and clinical research. As technology advances rapidly especially with the advent of AI in radiotherapy planning and radiomics in imaging the need for medically grounded physicists who understand both theory and practice becomes even more urgent. A culture that nurtures this dual identity is not only good for physicists, but also it is essential for patient centered innovation. With thoughtful support, flexible career paths, and strategic investment, medical physicists can thrive in both domains.
Medical physicists are vital members of modern healthcare teams, operating at the interface between science and clinical practice. They not only ensure safe and accurate delivery of radiation therapy and diagnostic imaging but also push the boundaries of technological innovation through research and development. However, the dual nature of this profession straddling clinical responsibilities and research aspirations poses challenges that institutions, professionals, and academic programs must address. This article explores the evolving role of the medical physicist, one mended between clinical and research commitments, and practical strategies for achieving a sustainable balance.
Clinical Service: The Unseen Backbone of Radiotherapy
In routine clinical settings, medical physicists are indispensable. Their primary duties include commissioning and calibrating radiation therapy equipment, performing patient specific quality assurance for radiation treatments, ensuring compliance with radiation safety regulations, routine treatment planning among many other works. These tasks are often time sensitive and demand meticulous attention. In radiotherapy departments, a physicist’s role is crucial in ensuring the correct dose is delivered to the right location with high accuracy since deviations in a patient’s plan or machine performance can lead to underdosing the tumor or over exposing healthy tissues. In high volume hospitals, especially in low- and middle-income countries, the clinical workload is always intense. A small team of physicists may be responsible for hundreds of patients per week, leaving little bandwidth for academic or research activities. This workload, while essential to patient care, can limit innovation if not managed effectively.
The Research Mandate: Driving the Future of Medical Physics
On the research front, medical physicists contribute to advancements in radiation oncology, imaging technology, dosimetry, artificial intelligence applications, and more. Research is the engine that drives improvement in treatment efficacy, patient safety, and workflow efficacy and efficiency. Medical physics is not static; each advancement in treatment hardware, therapy software, or computing power introduces new questions that physicists are uniquely qualified to answer. However, this progress depends on time, funding, and institutional support resources often scarce in busy clinical environments.
The Academic Medical Physicist: Bridging Two Worlds
Academic medical physicists play a unique and essential role. Positioned in universities or teaching hospitals, they are typically involved in:
- Teaching graduate students and residents
- Supervising clinical training programs
- Conducting original research
- Collaborating with industry and clinical partners
These professionals are often the linchpin connecting clinical insights with theoretical innovation. For example, a clinical problem such as image drift in MRI-guided radiotherapy can be studied in a lab, modelled mathematically, and solved through interdisciplinary research. However, academic physicists also face time pressure from teaching loads, grant writing, and administrative duties. Without structured support and funding, their potential impact on both patient care and scientific advancement may be underutilized.
The Challenge: Time, Workload, and Institutional Culture
One of the greatest obstacles to balancing clinical and research responsibilities is time allocation. In many hospitals, the emphasis is almost exclusively on immediate clinical service, with research viewed as an optional extra. This creates a culture where research may be deprioritized, even though it is essential for long term clinical improvement. This imbalance can lead to “a missed opportunity to exploit the full potential of medical physicists.” It called for formal recognition of research as an integral part of a physicist’s role, with corresponding adjustments in workload and performance metrics.
Strategies for Balance: Recommendations and Solutions
1. Protected Research Time
Hospitals and cancer centers should allocate defined blocks of time for research. Whether one day per week or 20% of total workload, this “protected time” allows physicists to engage in scientific inquiry without clinical pressure.
2. Dual Track Career Models
Institutions can offer parallel career paths, one with a clinical emphasis and another focused on research. This allows professionals to pursue their strengths while contributing meaningfully to the field.
3. Collaborative Research Models
Physicists can co-lead clinical trials or work with radiation oncologists, radiologists, and data scientists to address practical clinical challenges. Embedding research into clinical operations allows for real-world impact and greater feasibility.
4. Investment in Staff and Resources
In high workload centers, hiring additional staff or delegating non-specialist tasks (e.g., administrative reporting) can free up physicists for innovation. Using automation and AI for QA can also reduce repetitive burdens.
5. Academic Clinical Partnerships
Stronger ties between universities and hospitals can provide access to research infrastructure (e.g., labs, computing clusters) and students, creating an ecosystem where ideas move fluidly from bench to bedside.
The Way Forward: Recognizing Value Beyond Service
Medical physicists are more than simple clinical occupational workers, they are innovators, educators, and leaders in the fight against cancer. To fully harness their potential, both clinical institutions and academic centers must invest in integrated roles that value both clinical service and clinical research. As technology advances rapidly especially with the advent of AI in radiotherapy planning and radiomics in imaging the need for medically grounded physicists who understand both theory and practice becomes even more urgent. A culture that nurtures this dual identity is not only good for physicists, but also it is essential for patient centered innovation. With thoughtful support, flexible career paths, and strategic investment, medical physicists can thrive in both domains.
Managing Healthcare Waste in Developing Nations: A Growing Public Health Challenge
Dinelka Rasnayake
Department of Engineering Technology, Faculty of Technology, General Sir John Kotelawala Defence University, Sri Lanka
Healthcare waste (HCW), or medical waste, encompasses all waste generated by healthcare activities, from hospitals and clinics to laboratories and home care [1]. While approximately 85% of HCW is general, non- hazardous waste, the remaining 15% is classified as hazardous. This hazardous fraction includes infectious materials, sharps, pharmaceutical waste, chemical waste, and radioactive waste. Improper management poses severe risks to human health and the environment [1]. A critical issue in low-income countries is the lack of waste segregation. This leads to contamination of general waste, with hazardous waste in some facilities like those in Ethiopia reaching 62.74%, well above World Health Organization (WHO) standards [2]. HCW makes up about 1–2% of urban waste globally [1]. Waste generation is projected to grow by 73%, reaching 3.8 billion tonnes by 2050, significantly affecting low- and middle-income countries [3]. The economic cost could rise from USD 361 billion in 2020 to USD 640.3 billion by 2050. However, a shift to circular economy practices could yield a net benefit of USD 108.5 billion annually [3].
Why the Crisis is Deepening in Developing Countries
- Inadequate Infrastructure and Technology Access
Many developing countries lack the infrastructure and technology required for safe HCW management. Hospitals often do not have incinerators or autoclaves, leading to unsafe practices such as open burning or unregulated landfilling [1,4]. Table 1 presents a summary of hazardous waste generation rates (kg/bed/day) for various countries and income categories. Though low-income countries generate less hazardous waste up to 0.2 kg/bed/day compared to 0.5 kg in high-income countries, the poor segregation practices recorded in these low-income countries make much of this waste remains untreated [1].
Country | Hazardous Waste Generation Rate (kg/bed/day) |
High-income countries | Up to 0.5 |
Low-income countries | Up to 0.2 |
India | 0.8–2.31 |
China | 0.6–4.03 |
Ethiopia | 1.1–1.8 |
Kazakhstan | 5.34–5.4 |
Table 1:Hazardous Waste Generation Rate (kg/bed/day) in Various Nations
Inadequate Infrastructure and Technology Access
Many developing countries lack the infrastructure and technology required for safe HCW management. Hospitals often do not have incinerators or autoclaves, leading to unsafe practices such as open burning or unregulated landfilling [1,4]. Table 1 presents a summary of hazardous waste generation rates (kg/bed/day) for various countries and income categories. Though low-income countries generate less hazardous waste up to 0.2 kg/bed/day compared to 0.5 kg in high-income countries, the poor segregation practices recorded in these low-income countries make much of this waste remains untreated [1].
Ø Severe Financial Constraints
Healthcare systems in low-income countries prioritize clinical care over waste treatment. Public hospitals operate under strict budgets, and international funds are limited. The Global Fund allocated just 0.3% to HCW management (HCWM), and many COVID-19 responses spent less than 1% on waste management [6,4].
Ø Low Awareness and Unsafe Practices
Healthcare workers often lack awareness of HCW risks. In Ethiopia, 60.3% of staff experienced needlestick injuries, and across 22 developing nations, only 41% of workers received training [7,8]. Manual sorting without personal protective equipment (PPE) is widespread, increasing exposure to infections.
Ø Weak Regulatory Frameworks
Enforcement of regulations is weak. For instance, Bangladesh’s 2008 HCWM rules included provisions for a central authority which was never established [9]. In India, rural regions show poor compliance, and waste disposal is often outsourced to unlicensed contractors [10].
Informal waste workers operate without legal protections or PPE, leading to respiratory illnesses, infections, and reproductive disorders [3]. These workers are usually marginalized and excluded from formal waste management systems.
Ø Worsening Conditions such as Population Growth and Pandemics
Urbanization, population growth, and pandemics are rapidly increasing waste volumes. Waste generation in low-income countries is projected to triple by 2050 [3]. COVID-19 drastically increased plastic waste, further straining weak HCWM systems [11].
Pathways to Progress Towards Sustainable Healthcare Waste Management
Improper HCWM leads to disease spread such as human immuno-deficiency virus (HIV), Hepatitis, tuberculosis (TB), and cholera. Annually, 16 billion injections are administered, many without proper disposal. Poor HCWM contributes to 5.2 million deaths per year [12].
Environmental damage includes soil and water contamination from pharmaceuticals, open burning emissions (e.g., dioxins, furans), and microplastics. Sri Lanka emits 17.070 g TEQ (Toxic Equivalent Quantity) annually from small facilities and 179 kg of mercury per year [13,14]. Table 2 outlines key strategies and practical steps recommended for achieving sustainable HCWM, with regional examples and global best practices.
Step | Description | Examples / Remarks |
Segregation at Source | Use color-coded bins to separate waste types (e.g., yellow for biohazards, brown for radioactive, black for general). | Reduces hazardous volume; implementation still inconsistent despite growing awareness [15]. |
Onsite Treatment Solutions | Employ autoclaves, microwaves, and Sterilwave systems for decentralized treatment. | Suitable for low-resource areas; Sri Lanka’s incinerators often remain inefficient [16]. |
Training & Capacity Building | Continuous training for HCW handlers enhances safety and compliance. | WHO and United Nations Development Programme (UNDP) have run effective programs in South Asia [5]. |
Public-Private Partnerships (PPP) | PPPs can improve infrastructure and innovation. | Sri Lanka set national benchmarks; Nepal’s World Bank-funded PPPs expanded waste coverage to 70% [17,18]. |
Stronger Policies & Monitoring | Enforceable waste policies and tracking systems are essential. | India (2024 rules) uses audits/digital tracking; Bangladesh lags in enforcement [3,9]. |
Circular Economy Models | Convert waste to resources through recycling and energy recovery. | Tribhuvan Hospital (Nepal) reduced costs via recycling; aligns with United Nation’s Environment Programme (UNDP) 2024 recommendations [14,19]. |
Innovation & Best Practices | New technologies like solar- powered autoclaves and Sterilwave improve efficiency. | Developed by MIT/IIT and others for rural/urban needs [20]. |
Community Involvement | Engage local communities and cooperatives in HCWM activities. | Nepal & Sri Lanka initiatives support hygiene and livelihoods; e.g., biogas use at Tribhuvan Hospital [14]. |
Global Support | International agencies offer funding, tools, and training. | WHO, UNDP, UNEP, World Bank invested $5.13 billion in solid waste projects (2003– 2021) [3]. |
Table 2: Key Steps for Sustainable Healthcare Waste Management (HCWM)
Final Note
Effective healthcare waste management is no longer optional, it is essential for protecting public health, the environment, and future generations. With coordinated efforts across policy, technology, education, and community engagement, countries like Sri Lanka and its neighbors can transition toward safer, more sustainable HCWM systems. Global support and regional innovation must continue to drive this progress.
Reference List
- World Health Organization (WHO). Global Healthcare Waste Management 2022.
- Tadesse Healthcare waste generation and quantification in public health centres in Addis Ababa, Ethiopia. PLoS One. 2024;19(2):e0295165.
- Kaza, , Yao, L., Bhada-Tata, P. and Van Woerden, F., 2018. What a waste 2.0: a global snapshot of solid waste management to 2050. World Bank Publications.
- Partnership for Supply Chain Management (PFSCM). Status of Waste Treatment Technology in LMIC Hospitals. 2023. Available from: https://www.pfscm.org
- United Nations Development Programme (UNDP). Safe Healthcare Waste Management in the Global South. 2023. Available from: https://www.undp.org
- Global Fund. Waste Management in COVID-19 Response Projects. 2023. Available from: https://www.theglobalfund.org
- Mengistu DA, Tolera ST. Prevalence of occupational exposure to needle-stick injury and associated factors among healthcare workers of developing countries: Systematic review. J Occup Health. 2020;62(1):e12179.
- Public Health Toxicology. Occupational Hazards of Healthcare Workers in Developing 2023. Available from: https://www.ph-toxicology.com
- Dhaka Tribune. Bangladesh’s Healthcare Waste Management: 15 Years On. 2023. Available from: https://www.dhakatribune.com
- Infection Control Challenges in India’s Healthcare Waste Disposal. 2023. Available from: https://www.infectioncontroltoday.com
- Medical Waste COVID-19 and the Plastic Waste Surge. 2023. Available from: https://www.medicalwastepros.com
- Rahman, M.M., Bodrud-Doza, M., Griffiths, M.D. and Mamun, M.A., 2020. Biomedical waste amid COVID-19: perspectives from Bangladesh. The Lancet Global Health, 8(10), p.e1262.
- UNDP Sri Healthcare Waste Emissions in Sri Lanka. 2023. Available from: https://www.lk.undp.org
- United Nations Environment Programme (UNEP). Turning Waste Into Resources: Circular Economy in Healthcare. 2024. Available from: https://www.unep.org/resources/report/circular-healthcare-2024
- American Public Health Association (APHA). Healthcare Waste Segregation 2023. Available from: https://www.apha.org/HCW-Segregation
- Brighter Healthcare Waste Incineration in South Asia: A Regional Snapshot. 2025. Available from: https://www.brighterkashmir.com
- World Public-Private Models for Healthcare Waste Management. 2025. Available from: https://www.worldbank.org/en/news/feature/2025/02/20/ppp-models-healthcare-waste
- Healthcare Without Harm. Innovative Healthcare Waste Solutions in Nepal. 2024. Available from: https://www.noharm.org
- CCET (International Environmental Technology Centre). Healthcare Waste Management in Asia- Pacific. 2022. Available from: https://www.ccet.unep.org
- MIT MIT Develops Solar-Powered Autoclaves for Rural Clinics. 2020. Available from: https://news.mit.edu/2020/solar-autoclaves-developing-world
- Daniels Sterilwave Technology for Hospital Waste. 2024. Available from: https://www.danielshealth.com
Solve the Problem
Starting this issue, SCMPR Newsletter will carry a new column – SOLVE IT! – featuring a relatively difficult question / interesting problem for the young medical physics students and young medical physicists to solve. Those who are interested can send their answers to sptgnadar@gmail.com . The best answer would get published in the next issue of the Newsletter along with the name and affiliation of the contributor.
- A patient has to be treated by a direct 6 MV posterior spinal field of size 6 cm (width) x 48 cm (length) at an extended SSD of 120 cm. The prescribed dose is 1.8 Gy at a depth of 5.5 cm.
Data (output at dmax for 100 cm SSD, TMR) are given in the tables below. Using ONLY the data given in the tables, find out the treatment MUs.
Note: For equivalent square field, use the formula: Side of the square = 4*(area/perimeter)
6 MV photons – Output at the depth (dmax) of dose maximum (SSD = 100 cm) [Output (cGy/100 MU) is given at a depth of 1.5 cm in phantom, i.e. at a distance of 101.5 cm from the source] | |||||||||
Equivalent square side (cm) à | 7 | 7.5 | 8 | 8.5 | 9 | 9.5 | 10 | 10.5 | 11 |
cGy/100 MU à | 96.3 | 97.0 | 97.6 | 98.2 | 98.7 | 99.4 | 100.0 | 100.4 | 100.8 |
6 MV photons – TMR data for selected field sizes | |||||||||
Depth (cm) | Equivalent square field size (cm x cm) | ||||||||
6×6 | 7×7 | 8×8 | 9×9 | 10×10 | 11×11 | 12×12 | 13×13 | 14×14 | |
4.0 | 0.944 | 0.949 | 0.951 | 0.952 | 0.953 | 0.954 | 0.954 | 0.955 | 0.957 |
4.5 | 0.928 | 0.931 | 0.934 | 0.935 | 0.936 | 0.937 | 0.938 | 0.940 | 0.942 |
5.0 | 0.912 | 0.914 | 0.916 | 0.918 | 0.919 | 0.921 | 0.922 | 0.925 | 0.927 |
5.5 | 0.895 | 0.898 | 0.901 | 0.903 | 0.906 | 0.908 | 0.911 | 0.914 | 0.917 |
6.0 | 0.878 | 0.883 | 0.886 | 0.889 | 0.892 | 0.896 | 0.899 | 0.903 | 0.906 |